A 5-week-old infant presents with a 1-week history of progressive nonbilious emesis, associated with a 24hour history of decreased urine output. The infant continues to be active and eager to feed. On examination, the infant has a sunken fontanelle and decreased skin turgor. The abdomen is scaphoid, and with a test feed, there is a visible peristaltic wave in the epigastrium. Which of the following is the most appropriate next step in management of this infant?
A. immediate surgical exploration
B. send the child home with an oral electrolyte rehydration solution
C. change the infant's formula and feeding regimen
D. IV fluid resuscitation, followed by surgical intervention
E. initiate therapy with a prokinetic agent
Correct Answer: D
Infants with pyloric stenosis usually present after the third week of life with symptoms of progressive pyloric outlet obstruction secondary to increasing hypertrophy of the pyloric muscle. There are often clinical signs of dehydration, but the infant usually appears well and is eager to feed. Viral gastroenteritis and urinary tract sepsis may be associated with signs of such systemic illness as lethargy, poor feeding, and, in some cases, fever. Gastroesophageal reflux more typically presents with a history of regurgitation since birth. Milk protein allergy is often associated with colicky abdominal pain and diarrhea. The pathognomonic sign on clinical examination is a palpable "olive" in the epigastrium or right upper quadrant. Abdominal ultrasound is operator dependent, but with expertise in interpretation of the study, the thickened elongated pyloric channel can be demonstrated. AUGI contrast study may show the classic "shouldering" of the pyloric muscle, with a "string sign"; this also requires expertise in performing the examination, and other causes of pyloric outlet obstruction, such as pylorospasm may be misinterpreted as a positive study. Surgical exploration should be reserved for those patients in whom the diagnosis has been confirmed and only after the infant has received fluid resuscitation. Infants with gastric outlet obstruction develop a hypochloremic, hypokalemic metabolic alkalosis. This is secondary to the loss of chloride in the gastric contents, and the renal reabsorption of sodium in exchange for potassium and hydrogen. Carbonic anhydrase converts carbonic acid to hydrogen and bicarbonate ions, allowing hydrogen to be excreted in the urine, with retention of the bicarbonate. Hence, with the metabolic alkalosis, there is a "paradoxical aciduria." Hypernatremic, hyperchloremic, hypokalemic metabolic acidosis develops in infants with diarrhea. Infants with gastroesophageal reflux do not usually develop significant electrolyte derangements. Infants with pyloric stenosis will usually require a period offluid resuscitation to correct hypovolemia as well as electrolyte and acid-base abnormalities.
This is followed by a pyloromyotomy. Infants with vomiting and diarrhea from viral gastroenteritis are often successfully managed with oral rehydration. Prokinetic agents have been used in the management of gastroesophageal reflux. Soy formulas or elemental formulas are recommended for the infant with a milk protein allergy
Question 182:
A 5-week-old infant presents with a 1-week history of progressive nonbilious emesis, associated with a 24hour history of decreased urine output. The infant continues to be active and eager to feed. On examination, the infant has a sunken fontanelle and decreased skin turgor. The abdomen is scaphoid, and with a test feed, there is a visible peristaltic wave in the epigastrium. Electrolytes and a urinalysis are evaluated. Which of the following laboratory findings are most likely to be seen in this patient?
A. Na 145, K 3.0, Cl 110, CO2 17, urine pH 8.0
B. Na 130, K 3.0, Cl 80, CO2 36, urine pH 4.0
C. Na 135, K 4.0, Cl 104, CO2 23, urine pH 7.0
D. Na 140, K 5.2, Cl 100, CO2 16, urine pH 4.0
E. Na 132, K 3.2, Cl 96, CO2 25, urine pH 7.0
Correct Answer: B
Infants with pyloric stenosis usually present after the third week of life with symptoms of progressive pyloric outlet obstruction secondary to increasing hypertrophy of the pyloric muscle. There are often clinical signs of dehydration, but the infant usually appears well and is eager to feed. Viral gastroenteritis and urinary tract sepsis may be associated with signs of such systemic illness as lethargy, poor feeding, and, in some cases, fever. Gastroesophageal reflux more typically presents with a history of regurgitation since birth. Milk protein allergy is often associated with colicky abdominal pain and diarrhea. The pathognomonic sign on clinical examination is a palpable "olive" in the epigastrium or right upper quadrant. Abdominal ultrasound is operator dependent, but with expertise in interpretation of the study, the thickened elongated pyloric channel can be demonstrated. AUGI contrast study may show the classic "shouldering" of the pyloric muscle, with a "string sign"; this also requires expertise in performing the examination, and other causes of pyloric outlet obstruction, such as pylorospasm may be misinterpreted as a positive study. Surgical exploration should be reserved for those patients in whom the diagnosis has been confirmed and only after the infant has received fluid resuscitation. Infants with gastric outlet obstruction develop a hypochloremic, hypokalemic metabolic alkalosis. This is secondary to the loss of chloride in the gastric contents, and the renal reabsorption of sodium in exchange for potassium and hydrogen. Carbonic anhydrase converts carbonic acid to hydrogen and bicarbonate ions, allowing hydrogen to be excreted in the urine, with retention of the bicarbonate. Hence, with the metabolic alkalosis, there is a "paradoxical aciduria." Hypernatremic, hyperchloremic, hypokalemic metabolic acidosis develops in infants with diarrhea. Infants with gastroesophageal reflux do not usually develop significant electrolyte derangements. Infants with pyloric stenosis will usually require a period offluid resuscitation to correct hypovolemia as well as electrolyte and acid-base abnormalities.
This is followed by a pyloromyotomy. Infants with vomiting and diarrhea from viral gastroenteritis are often successfully managed with oral rehydration. Prokinetic agents have been used in the management of gastroesophageal reflux. Soy formulas or elemental formulas are recommended for the infant with a milk protein allergy
Question 183:
A 5-week-old infant presents with a 1-week history of progressive nonbilious emesis, associated with a 24hour history of decreased urine output. The infant continues to be active and eager to feed. On examination, the infant has a sunken fontanelle and decreased skin turgor. The abdomen is scaphoid, and with a test feed, there is a visible peristaltic wave in the epigastrium. Which of the following is the most likely diagnosis?
A. viral gastroenteritis
B. gastroesophageal reflux
C. urinary tract sepsis
D. pyloric stenosis
E. milk protein allergy
Correct Answer: D
Infants with pyloric stenosis usually present after the third week of life with symptoms of progressive pyloric outlet obstruction secondary to increasing hypertrophy of the pyloric muscle. There are often clinical signs of dehydration, but the infant usually appears well and is eager to feed. Viral gastroenteritis and urinary tract sepsis may be associated with signs of such systemic illness as lethargy, poor feeding, and, in some cases, fever. Gastroesophageal reflux more typically presents with a history of regurgitation since birth. Milk protein allergy is often associated with colicky abdominal pain and diarrhea. The pathognomonic sign on clinical examination is a palpable "olive" in the epigastrium or right upper quadrant. Abdominal ultrasound is operator dependent, but with expertise in interpretation of the study, the thickened elongated pyloric channel can be demonstrated. AUGI contrast study may show the classic "shouldering" of the pyloric muscle, with a "string sign"; this also requires expertise in performing the examination, and other causes of pyloric outlet obstruction, such as pylorospasm may be misinterpreted as a positive study. Surgical exploration should be reserved for those patients in whom the diagnosis has been confirmed and only after the infant has received fluid resuscitation. Infants with gastric outlet obstruction develop a hypochloremic, hypokalemic metabolic alkalosis. This is secondary to the loss of chloride in the gastric contents, and the renal reabsorption of sodium in exchange for potassium and hydrogen. Carbonic anhydrase converts carbonic acid to hydrogen and bicarbonate ions, allowing hydrogen to be excreted in the urine, with retention of the bicarbonate. Hence, with the metabolic alkalosis, there is a "paradoxical aciduria." Hypernatremic, hyperchloremic, hypokalemic metabolic acidosis develops in infants with diarrhea. Infants with gastroesophageal reflux do not usually develop significant electrolyte derangements. Infants with pyloric stenosis will usually require a period offluid resuscitation to correct hypovolemia as well as electrolyte and acid-base abnormalities.
This is followed by a pyloromyotomy. Infants with vomiting and diarrhea from viral gastroenteritis are often successfully managed with oral rehydration. Prokinetic agents have been used in the management of gastroesophageal reflux. Soy formulas or elemental formulas are recommended for the infant with a milk protein allergy
Question 184:
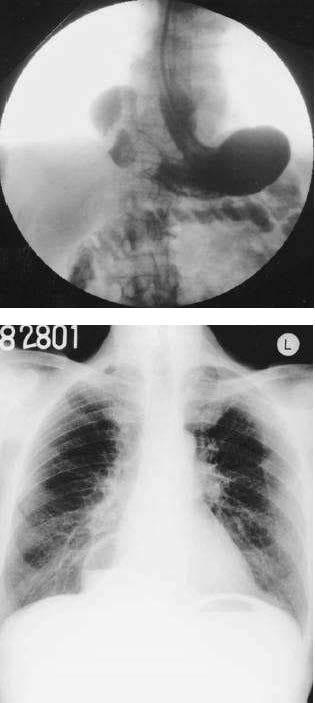
An 85-year-old man presents to the emergency room with an acute onset of midepigastric pain, nausea, vomiting, and hiccups starting 2 days ago. He is unable to keep any food down. Past history is pertinent for a long-standing hiatal hernia, hypertension, and diet-controlled diabetes. Examination reveals vital signs of pulse rate 82/min, BP 100/52 mmHg, respiratory rate 16/min, and temperature 97.2°F. The patient is in no acute distress, but has epigastric tenderness without guarding. Laboratory analysis revealed a hematocrit of 46 and a normal white blood cell (WBC) count. A chest x-ray is shown in Figure. A fluoroscopically guided NG tube was placed using contrast, and his stomach was decompressed.After adequate fluid and electrolyte resuscitation, an upper gastrointestinal (UGI) contrast study was obtained and is shown in Figure.
Which of the following is the most appropriate next step in management?
A. laparotomy or laparoscopy and operative repair
B. continued NG tube decompression and initiation of total parenteral nutrition (TPN)
C. thoracotomy or thoracoscopy and operative repair
D. endotracheal intubation and initiation of ventilatory support
E. upper endoscopy
Correct Answer: A
The most likely diagnosis based on the chest xray and UGI contrast study is a paraesophageal hernia involving the gastric antrum and proximal duodenum. Although some contrast is seen in the transverse colon from that used during fluoroscopic placement of the NG tube, most of the contrast in the UGI study does not leave the stomach and proximal duodenum, suggesting some degree of obstruction. A sliding hiatal hernia involves movement of the gastroesophageal junction into the mediastinum above the diaphragmatic hiatus. The figure shows the gastroesophageal junction below the diaphragmatic hiatus. Hernias of Bochdalek and Morgagni are congenital diaphragmatic hernias involving the posterorlateral and parasternal locations, respectively. Eventration is an attenuation of the central portion of the diaphragm with resultant upward displacement. The most appropriate treatment is laparotomy or laparoscopy with reduction of the hernia and repair. Thoracotomy or thoracoscopy would not allow easy access to the abdominal contents and is associated with increased morbidity. Delaying surgery may result in strangulation and ischemia. Because the patient did not demonstrate any respiratory compromise, endotracheal intubation was not indicated. Endoscopy is useful to evaluate for mucosal erosions in the case of gastrointestinal bleeding
Question 185:
An 85-year-old man presents to the emergency room with an acute onset of midepigastric pain, nausea, vomiting, and hiccups starting 2 days ago. He is unable to keep any food down. Past history is pertinent for a long-standing hiatal hernia, hypertension, and diet-controlled diabetes. Examination reveals vital signs of pulse rate 82/min, BP 100/52 mmHg, respiratory rate 16/min, and temperature 97.2°F. The patient is in no acute distress, but has epigastric tenderness without guarding. Laboratory analysis revealed a hematocrit of 46 and a normal white blood cell (WBC) count. A chest x-ray is shown in Figure. A fluoroscopically guided NG tube was placed using contrast, and his stomach was decompressed.After adequate fluid and electrolyte resuscitation, an upper gastrointestinal (UGI) contrast study was obtained and is shown in Figure. Which of the following is the most likely diagnosis?
A. sliding hiatal hernia
B. hernia of Bochdalek (posterorlateral congenital diaphragmatic hernia)
C. hernia of Morgagni (parasternal congenital diaphragmatic hernia)
D. paraesophageal hernia
E. eventration of the diaphragm (central diaphragm)
Correct Answer: D
The most likely diagnosis based on the chest xray and UGI contrast study is a paraesophageal hernia involving the gastric antrum and proximal duodenum. Although some contrast is seen in the transverse colon from that used during fluoroscopic placement of the NG tube, most of the contrast in the UGI study does not leave the stomach and proximal duodenum, suggesting some degree of obstruction. A sliding hiatal hernia involves movement of the gastroesophageal junction into the mediastinum above the diaphragmatic hiatus. The figure shows the gastroesophageal junction below the diaphragmatic hiatus. Hernias of Bochdalek and Morgagni are congenital diaphragmatic hernias involving the posterorlateral and parasternal locations, respectively. Eventration is an attenuation of the central portion of the diaphragm with resultant upward displacement. The most appropriate treatment is laparotomy or laparoscopy with reduction of the hernia and repair. Thoracotomy or thoracoscopy would not allow easy access to the abdominal contents and is associated with increased morbidity. Delaying surgery may result in strangulation and ischemia. Because the patient did not demonstrate any respiratory compromise, endotracheal intubation was not indicated. Endoscopy is useful to evaluate for mucosal erosions in the case of gastrointestinal bleeding
Question 186:
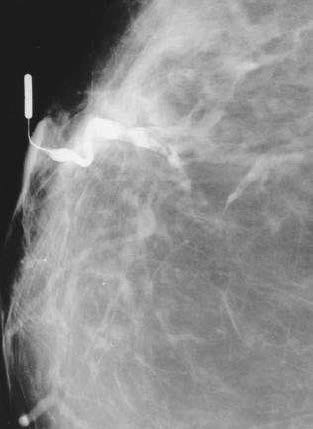
A 51-year-old woman presents to the physician's office with a 2-month history of a right breast bloodtinged nipple discharge. Past history is unremarkable. Family history is positive for postmenopausal breast cancer in a maternal grandmother. Examination reveals no palpable masses or regional adenopathy, but a serous discharge is easily elicited from a single duct in the right breast. Bilateral mammograms show no abnormalities. Cytology from the discharge was not diagnostic. A ductogram was ordered, and the results are shown in the figure below.
Which of the following is the most appropriate next step in management?
A. collection of discharge for repeat cytologic analysis
B. observation, with repeat examination and imaging studies in 36 months
C. modified radical mastectomy
D. central lumpectomy (including removal of the nipple/areolar complex)
E. terminal duct excision (microdochectomy)
Correct Answer: E
The most common cause of a nipple discharge is an intraductal papilloma. Galactography can often demonstrate a filling defect in the terminal ducts as is demonstrated in the figure. Duct ectasia may also cause a discharge, but the discharge is usually thick and pasty. Carcinoma is an uncommon cause of nipple discharge. The next step in management would be excision of the terminal duct containing the papilloma. Repeat cytology would not be useful because a negative result does not preclude biopsy. Observation would not be prudent, because a diagnosis of carcinoma must be excluded, and the papilloma may enlarge, requiring a more extensive operation at a later date. A more extensive operation, such as a central lumpectomy or mastectomy, would be unnecessary because the lesion is benign.
Question 187:
A 51-year-old woman presents to the physician's office with a 2-month history of a right breast bloodtinged nipple discharge. Past history is unremarkable. Family history is positive for postmenopausal breast cancer in a maternal grandmother. Examination reveals no palpable masses or regional adenopathy, but a serous discharge is easily elicited from a single duct in the right breast. Bilateral mammograms show no abnormalities. Cytology from the discharge was not diagnostic. A ductogram was ordered, and the results are shown in the figure below.
Which of the following is the most likely diagnosis?
A. invasive carcinoma
B. intraductal carcinoma
C. intraductal papilloma
D. fibrocystic disease
E. duct ectasia
Correct Answer: C
The most common cause of a nipple discharge is an intraductal papilloma. Galactography can often demonstrate a filling defect in the terminal ducts as is demonstrated in the figure. Duct ectasia may also cause a discharge, but the discharge is usually thick and pasty. Carcinoma is an uncommon cause of nipple discharge. The next step in management would be excision of the terminal duct containing the papilloma. Repeat cytology would not be useful because a negative result does not preclude biopsy. Observation would not be prudent, because a diagnosis of arcinoma must be excluded, and the papilloma may enlarge, requiring a more extensive operation at a later date. A more extensive operation, such as a central lumpectomy or mastectomy, would be unnecessary because the lesion is benign.
Question 188:
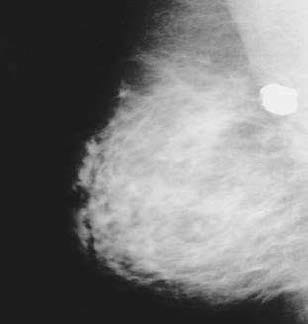
A 55-year-old-woman presents to the physician's office for evaluation of mammographic findings on a screening mammogram. She denies any breast masses, nipple discharge, pain, or skin changes. Past history is pertinent for insulin-dependent diabetes. Family history is positive for postmenopausal breast cancer in her mother. She has a normal breast examination and no axillary adenopathy. A mediolateral oblique (MLO) view of the right breast is shown in the figure below.
Which of the following is the most appropriate next step in management?
A. observation, with repeat mammogram in 612 months
B. ultrasound
C. biopsy
D. lumpectomy, radiation therapy, and sentinel lymph node (SLN) biopsy
E. total mastectomy
Correct Answer: A
The mammographic appearance of popcornlike, coarse calcifications in the breast is characteristic of an involuting, or degenerating fibroadenoma in a postmenopausal woman. Mammographic follow-up is appropriate. A repeat study at 6 months would be considered if no prior films are available in order to assess stability of a new mammographic finding. Though ultrasound is often performed for solid masses, the amount of calcification in the mass would lead to artifact, making interpretation difficult. Biopsy would not be suggested based on the characteristic mammographic findings. Other surgical procedures would not be indicated
Question 189:
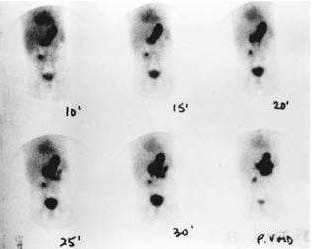
A2-year-old child presents with a 2-day history of painless rectal bleeding. On examination, the child is pale with tachycardia. The abdomen is nondistended and nontender. There is dark blood on rectal examination. The child has the following imaging study. Which of the following is the most appropriate management?
A. surgical exploration
B. aggressive resuscitation followed by surgical exploration
C. colonoscopy
D. acid suppression therapy
E. IV steroids
Correct Answer: B
Meckel's diverticulum typically presents in young children with painless rectal bleeding. The etiology of the bleeding is from ulceration of the adjacent ileum that is bathed by the acid produced from the ectopic gastric mucosa in the diverticulum. Bleeding may result in hypovolemia, requiring aggressive resuscitation before any surgical intervention. Diagnosis is made by technetium scan, with the child pretreated with H2 blocks to increase the sensitivity. Colonoscopy is reserved for those children with a negative Meckel's scan. Acid suppression therapy is not indicated. At surgical exploration, the diverticulum and adjacent ileum are removed.
Question 190:
A 55-year-old-woman presents to the physician's office for evaluation of mammographic findings on a screening mammogram. She denies any breast masses, nipple discharge, pain, or skin changes. Past history is pertinent for insulin-dependent diabetes. Family history is positive for postmenopausal breast cancer in her mother. She has a normal breast examination and no axillary adenopathy. A mediolateral oblique (MLO) view of the right breast is shown in the figure below.
Which of the following is the most likely diagnosis?
A. milk of calcium
B. lobular carcinoma in situ (LCIS) with or without an invasive component
C. ductal carcinoma in situ (DCIS) with or without an invasive component
D. involuting fibroadenoma
E. phyllodes tumor
Correct Answer: D
The mammographic appearance of popcornlike, coarse calcifications in the breast is characteristic of an involuting, or degenerating fibroadenoma in a postmenopausal woman. Mammographic follow-up is appropriate. A repeat study at 6 months would be considered if no prior films are available in order to assess stability of a new mammographic finding. Though ultrasound is often performed for solid masses, the amount of calcification in the mass would lead to artifact, making interpretation difficult. Biopsy would not be suggested based on the characteristic mammographic findings. Other surgical procedures would not be indicated.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.