A 39-year-old pregnant woman with chronic hypertension and one prior pregnancy is now at 38 weeks' gestation. She comes to labor and delivery with profuse vaginal bleeding and abdominal pain of sudden onset.
This patient has an external fetal monitor placed. Uterine tone seems to be increased, and there are occasional variable decelerations of the fetal heart to 90 BPM. Which of the following is the most appropriate management?
A. tocolysis with a -receptor agonist
B. Pitocin induction of labor
C. continued monitoring of mother and baby
D. amniotomy
E. cesarean section
Correct Answer: E
At term, a placental abruption severe enough to cause fetal distress warrants immediate delivery. If the pregnancy is remote from term, temporizing measures may be considered, such as observation. However, delivery should be achieved if the mother becomes hemodynamically unstable. Tocolysis is ineffective in relaxing the uterus and has the added disadvantage of causing vasodilation of an already under-filled vascular system. Amniotomy and Pitocin induction will not cause delivery rapidly enough to prevent further deterioration of the fetus. Evidence of fetal distress makes continued monitoring unacceptable.
Question 552:
A 39-year-old pregnant woman with chronic hypertension and one prior pregnancy is now at 38 weeks'
gestation. She comes to labor and delivery with profuse vaginal bleeding and abdominal pain of sudden
onset.
If the patient has a placental abruption, which of the following is the most likely risk factor
A. advanced maternal age
B. low parity
C. coitus immediately before the onset of bleeding
D. hypertension
E. a step aerobic class immediately before the onset of bleeding
Correct Answer: D
Maternal hypertension is the most common risk factor for a placental abruption. The relative risk is 3.8 for parous women and 1.6 for nulliparous women. In one published report, half of the women with an abruption severe enough to kill the fetus had hypertension, and half of these had evidence of chronic vascular disease. Advanced maternal age without confounding factors such as diabetes or hypertension is not a risk factor for placental abruption. High parity is associated with an increased risk of placental abruption. Vigorous coitus can cause a vaginal laceration, but not abdominal pain. While blunt abdominal trauma may cause a placental abruption, routine forms of exercise are not a risk factor for placental abruption.
Question 553:
A 39-year-old pregnant woman with chronic hypertension and one prior pregnancy is now at 38 weeks' gestation. She comes to labor and delivery with profuse vaginal bleeding and abdominal pain of sudden onset.
Which of the following is the most likely diagnosis?
A. bloody show
B. vaginal laceration from coitus
C. cervicitis
D. placenta previa
E. placental abruption
Correct Answer: E
Painful vaginal bleeding is most likely the result of placental abruption, premature separation of the placenta. Bloody show is a normal sign of impending or early labor. The bleeding is scant and intermingled with clear mucus. Bleeding from a vaginal laceration following coitus is not associated with abdominal pain. A history of coitus followed immediately by bleeding suggests this diagnosis. Bleeding from cervicitis is most often spotting and not associated with abdominal pain. Classically, bleeding with a placenta previa is painless.
Question 554:
A healthy 27-year-old male and his partner have been attempting to conceive for more than 1 year. As part of their evaluation he has a semen analysis. His ejaculate volume is 3.5 mL, sperm concentration is 8 million/mL, sperm motility is 65%, oval forms comprise 60% of the sperm, and fructose is present in the ejaculate. The man is treated with clomiphene for a presumptive diagnosis of male factor infertility. Though clomiphene is an unproven and unapproved therapy for male infertility, what is the earliest that a semen analysis should be done to detect an improvement in his semen parameters?
A. 33 days
B. 53 days
C. 73 days
D. 90 days
E. 120 days
Correct Answer: D
The cycle of spermatogenesis is 73 ?5 days. This is the time required for maturation of spermatogonia to spermatozoa. The cycle is at different stages along the seminiferous tubules, necessary to ensure the presence of sperm in each ejaculate. Further, spermatozoa require approximately 3 weeks to traverse the ductal system and appear in the ejaculate. Knowing this has important implications: any therapy intended to stimulate spermatogenesis must be continued for at least the duration of one spermatogenic cycle to determine whether there is a beneficial effect. While impaired spermatogenesis may occur late in the cycle of spermatogenesis and improvement with clomiphene may occur sooner, the semen analysis should still be delayed for 90 days to provide better evidence for the presence or absence of improvement in the semen analysis. Results must be interpreted with caution because there is great biological variability in semen parameters: what is interpreted as a therapeutic effect may only be natural biological variation. Ultimately, pregnancy is the only meaningful measure of treatment success
and pregnancy may have occurred despite the therapy, not because of it.
Question 555:
A healthy 27-year-old male and his partner have been attempting to conceive for more than 1 year. As part of their evaluation he has a semen analysis. His ejaculate volume is 3.5 mL, sperm concentration is 8 million/mL, sperm motility is 65%, oval forms comprise 60% of the sperm, and fructose is present in the ejaculate. Which of these semen parameters is abnormal and suggests that this couple's infertility may be due to a male factor?
A. ejaculate volume
B. sperm concentration
C. sperm motility
D. sperm morphology
E. presence of fructose
Correct Answer: B
The WHO suggests a minimal sperm concentration of 20 million/mL for normal conception rates of 1520% per ovulation. However, sperm motility (percentage and velocity; >50% with forward progression), sperm morphology (30% or more oval forms, using strict criteria), coital frequency, and others must be considered. Stated otherwise, a sperm concentration of 10 million/mL may be associated with normal fertility if the sperm motility and morphology are better than average and coital frequency is three to four times per week. Any abnormality of a semen analysis should be confirmed by a repeat semen analysis no sooner than 4 weeks after the initial analysis.
Question 556:
A 37-year-old man and his wife seek help for their 5-year history of primary infertility. Her infertility investigation is normal. However, the husband has an ejaculate volume of 0.4 mL, and there are no sperm in the ejaculate. Aqualitative test for fructose in the semen is negative. Which of the following is the most likely diagnosis?
A. germ cell aplasia
B. bilateral occlusion of the vasa deferentia
C. 17-hydroxylase deficiency
D. congenital absence of the vasa deferentia
E. Klinefelter syndrome
Correct Answer: D
The normal ejaculate volume is 25 mL, and the bulk of the ejaculate is from the seminal vesicles. The reduced ejaculate volume may be the result of an incomplete collection or may indicate absence of the seminal vesicles. Fructose is the reducing sugar produced by the seminal vesicles, and its absence establishes a diagnosis of congenital bilateral absence of the vasa deferentia and seminal vesicles. This explains the azoospermia (absence of sperm; aspermia is absence of an ejaculate). Men with germ cell aplasia have only Sertoli cells in their seminiferous tubules. Their ejaculate volumes are normal, and fructose is present. Likewise, men with occlusion of the vasa deferentia will be azoospermic but have a normal ejaculate volume containing fructose. Men with 17- hydroxylase deficiency will have hypertension, be sexually infantile, and have azoospermia, because the enzyme deficiency prevents the secretion of normal amounts of cortisol, androgens, and estrogen, but an increased secretion of mineralocorticoids. Men with Klinefelter syndrome have patent vasa deferentia and seminal vesicles; their ejaculate volumes will be normal and contain fructose.
Question 557:
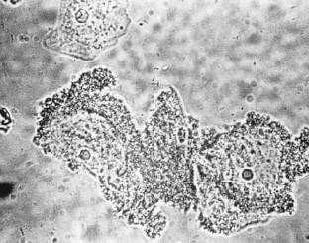
A wet smear of a vaginal discharge is illustrated in Figure.Which of the following is the most likely cause of the discharge?
Which of the following is the most appropriate treatment for the discharge illustrated in Figure?
A. clindamycin
B. erythromycin
C. metronidazole
D. miconazole
E. doxycycline
Correct Answer: C
The treatment of choice for bacterial vaginosis is metronidazole, also an effective treatment for trichomonas vaginitis. The dose is 375500 mg orally twice daily for 1 week. A single daily dose of 750 mg was recently approved. Vaginal metronidazole gel or clindamycin cream are also approved forms of treatment. Concurrent therapy of the male partner is controversial. Treatment in pregnancy is recommended, because there is a potential association of bacterial vaginosis and preterm labor and delivery.
Question 558:
A wet smear of a vaginal discharge is illustrated in Figure.Which of the following is the most likely cause of the discharge?
A. monilial vaginitis
B. trichomonas vaginitis
C. Chlamydia trachomatis
D. N. gonorrhoeae
E. bacterial vaginosis
Correct Answer: E
Clue cells are shown in Figure. This indicates bacterial vaginosis. Clue cells are vaginal squamous cells with indistinct margins that are studded extensively with coccobacilli. Trichomonas infection is caused by a unicellular protozoon. The organism on wet smear with normal saline is fusiform, slightly larger than white blood cells, and has flagella at one end. The flagella cause the motion on wet smear that is diagnostic. Monilial vaginitis is best demonstrated by placing a small amount of the discharge in 10% KOH and observing for branching hyphae. N. gonorrhoeae and C. trachomatis cannot be seen on a wet smear.
Question 559:
A 26-year-old woman complains of a vaginal discharge causing burning and itching of the perineum. The pH of the discharge is 4.5. Which of the following is the most likely cause of her discharge?
A. monilial vaginitis
B. trichomonas vaginitis
C. chlamydial cervicitis
D. gonococcal cervicitis
E. bacterial vaginosis
Correct Answer: A
The normal pH of the vagina is 3.84.2. In women with a vaginal discharge, a pH less than 5.0 suggests monilial vaginitis or a physiologic discharge of normal squamous cells desquamated from the vaginal epithelium. A pH greater than 5.0 suggests some type of bacterial infection, such as bacterial vaginosis or trichomonas vaginitis. The diagnosis of bacterial vaginosis is based on the presence of 3 of 4 characteristics: pH greater than 4.5, a homogenous thin appearance of the vaginal discharge, a fishy amine odor after the addition of 10% potassium hydroxide (KOH) to the discharge, and clue cells present in 2050% of vaginal epithelial cells. Clue cells are bacteria adherent to the surface of vaginal epithelial cells. Lactobacilli are absent from the vagina in women with bacterial vaginosis. Both chlamydia and gonorrhea infect the cervix and do not change the vaginal pH.
Question 560:
A couple consults you because each has neurofibromatosis and wish to know what their reproductive possibilities are. You should tell them which of the following?
A. The disease is lethal and results in spontaneous abortion of homozygous fetuses.
B. 25% of the females will be affected.
C. 50% of all offspring will be homozygous for the abnormal gene.
D. 75% or more of their offspring will have the disease.
E. 25% of their offspring will be unaffected.
Correct Answer: D
This is an autosomal dominant disorder. Both parents are carriers of the abnormal gene (N), which is on chromosome 17. If each parent is a heterozygote (Nn, where n is the normal gene), 25% of their offspring will have a normal genotype, nn. Fifty percent of their offspring will be affected heterozygotes (Nn), and the remaining 25% will be homozygous affected (NN). If either parent or both are homozygous for the abnormal gene (NN), 100% of the offspring will be affected. As an autosomal disorder, there is no sex predilection; males and females are affected with equal frequency. Prenatal diagnosis is available.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.