During a routine checkup, a 45-year-old executive is found to have hypercalcemia. Subsequent workup reveals elevated parathormone, decreased phosphorus, elevated chloride, and normal blood urea nitrogen (BUN), and creatinine in serum. Urinary calcium is above normal levels. What is the most likely etiology?
A. multiple myeloma
B. primary hyperparathyroidism
C. hypervitaminosis D
D. sarcoidosis
E. milk alkali syndrome
Correct Answer: B
Primary hyperparathyroidism is characterized by hypercalcemia, hypophosphatemia, hyperchloremia, increased urinary calcium excretion, and an increase in serum parathormone level. Multiple myeloma is associated with hypercalcemia when there are many lytic lesions. Chronic ingestion of 50100 times the normal requirement of vitamin D is required to produce hypercalcemia in normal people, so hypervitaminosis D is rare and parathormone levels would be suppressed. With milk alkali syndrome, which is caused by excess ingestion of calcium and absorbable antacids, parathormone levels would also be suppressed. In sarcoidosis, about 10% of patients have hypercalcemia attributable to increased intestinal absorption of calcium and increased production of 1,25(OH)2D.
Question 702:
In a patient infected with HIV, which of the following laboratory parameters provides the most useful information about the current immunologic status of the patient?
A. HIV RNA level
B. white blood cell (WBC) count
C. CD4+ T-cell count
D. CD8+ T-cell count
E. p24 antigen level
Correct Answer: C
The CD4+ T-cell count provides information on the current immunologic status of a patient infected with HIV. HIV RNA level measures viral load and predicts what will happen to the CD4+ count in the near future. WBC count is a nonspecific marker for infection. The p24 antigen assay is used for direct detection of HIV. CD8+ count typically is not as important in monitoring immunologic status though the CD4+/CD8+ ratio sometimes is used
Question 703:
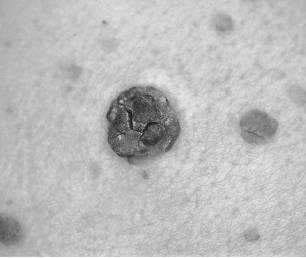
When you examine the back of an elderly gentleman, you note multiple brown papules and nodules having a "stuck on" appearance. These are shown in Figure. The patient tells you they have been there for years. Which of the following is the most likely diagnosis?
A. melanocytic nevi
B. actinic keratoses
C. seborrheic keratoses
D. seborrheic dermatitis
E. malignant melanoma
Correct Answer: C
This man has multiple seborrheic keratoses, which are very common, benign pigmented tumors that occur after age 30, especially on the trunk and face. Melanocytic nevi are usually small, circumscribed, pigmented macules or papules, rather than large "stuck-on" nodules. Actinic keratoses are red, scaly (not dark) lesions on the face and arms that are from suninduced damage. Seborrheic dermatitis is a red, scaly rash along the scalp, eyebrows, and nasolabial folds. Malignant melanoma would be in the differential if it were a single lesion.
Question 704:
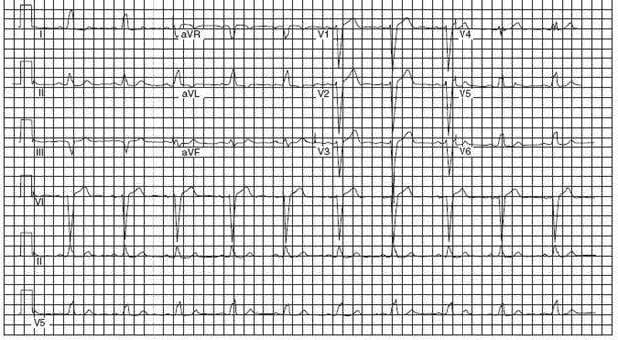
A 58-year-old man is establishing care with you because his insurance changed. His old records have not yet arrived, but he is complaining of palpitations and lightheadedness, so you order the ECG shown in Figure
Which of the following is the most likely problem associated with this pattern?
A. congenital heart disease
B. severe aortic valve disease
C. hypokalemia
D. atrial septal defect (ASD)
E. VSD
Correct Answer: B
The prolonged, negative QRS vector anteriorly (V1-V3) and wide notched R waves in V5 and V6 are characteristic for LBBB. In RBBB, there is an rSR' complex in V1 and QRS pattern in V6. Accelerated junctional rhythm would not have P waves. Partial blocks, such as left anterior fascicular block, generally do not prolong the QRS duration substantially, but are associated with shifts in the frontal plane QRS axis (left axis deviation). With intraventricular conduction delay, the QRS is between 100 and 120 ms. LBBB is a marker of one of four conditions: severe aortic valve disease, ischemic heart disease, long-standing hypertension, and cardiomyopathy. RBBB is seen more commonly than LBBB in patients without structural heart disease, although RBBB also occurs with congenital heart disease and ASD or valvular heart disease. Hyper- but not hypokalemia may cause intraventricular conduction delay. Myocarditis does not usually lead to LBBB.
Question 705:
A 30-year-old woman who has been human immunodeficiency virus (HIV) positive for 4 years was recently diagnosed with AIDS.
Which of the following immunologic abnormalities would be expected?
A. increased numbers of CD4+ (helper) T cells
B. decreased number of CD8+ (suppressor) T cells
C. cutaneous anergy to usual skin test antigens
D. normal B-cell function
E. increased natural killer cell function
Correct Answer: C
The new case definition for AIDS in 1993 added pulmonary tuberculosis, invasive cervical cancer, and recurrent pneumonia. This CDC classification system is divided into three categories: category A is symptomatic infection with HIV and includes acute illness and persistent lymphadenopathy; category B includes conditions attributed to HIV infection, such as oral thrush, herpes zoster, and peripheral neuropathy; category C is the AIDS surveillance cases. Anergy to common skin test antigens is a common finding with HIV infection. There is a decline in CD4 cell numbers, a relative increase in the number of T8 cells, which results in a decreased T4:T8 ratio of less than 1. Functional abnormalities occur in both B cells and natural killer cells, which accounts for the increase in certain bacterial infections seen in advanced HIV disease. Elevation of beta2 submicroglobulin, a serologic finding reflecting immunologic dysfunction, is a fairly reliable marker of progressive immunologic decline and the subsequent development of AIDS.
Question 706:
A 62-year-old man is undergoing neurologic evaluation. His arteriogram demonstrates the lesion shown in the figure below. Which of the following deficits is compatible with this lesion?
A. diplopia
B. transient monocular blindness
C. ataxia
D. vertigo
E. dysarthria
Correct Answer: B
The cerebral arteriogram shown in Figure reveals severe stenosis of the common carotid artery proximal to its bifurcation, as well as small lesions in the more distal vessels. Common manifestations are transient monocular blindness (amaurosis fugax), hemiparesis, hemisensory loss, aphasia, and homonymous visual field defects. Ataxia would be an unusual feature of carotid disease and, if present, would suggest involvement of the vertebrobasilar arteries, which results in dysarthria, diplopia, and vertigo.
Question 707:
A 35-year-old pharmacist complains of "hurting all over." Her pain is particularly bad in her upper back and shoulders, and she notes morning stiffness. On examination, her joints are not inflamed, but she has symmetric "tender points" in the posterior neck, anterior chest, lateral buttocks, medial knees, and lateral elbows. You make a preliminary diagnosis of fibromyalgia.
Which of the following is the most appropriate therapeutic recommendation?
A. avoid most physical activity
B. trial of amoxicillin
C. benzodiazepine in low doses for sleep
D. low-dose steroid
E. low-dose antidepressant
Correct Answer: E
Sleep disturbance is a characteristic symptom associated with fibromyalgia. Patients awaken feeling tired. The examination, other than tenderness in 14 specific, symmetrical points, is usually normal. Fever, rash on the extremities, muscle weakness, and migratory joint inflammation point to Lyme disease or other rheumatologic disorders. Asedimentation rate should be normal. If elevated, it may point to another diagnosis. Lyme titers are not indicated unless the patient has symptoms or history suggestive of the disease. Electromyelography and spine radiographs are typically normal and unnecessary for help in establishing the diagnosis. Depression can be associated with pain, but screening for it early on does not make sense and might offend the patient. Low-dose antidepressants often help to correct the sleep pattern and result in relief of pain. Nonsteroidal anti-inflammatory agents can also be used as needed; low-dose steroid is not indicated. Exercise is also helpful, and patients should be encouraged to stay physically active. Amoxicillin is not used for fibromyalgia. Benzodiazepines have addictive potential and lose their effectiveness for sleep after a few weeks.
Question 708:
A 35-year-old pharmacist complains of "hurting all over." Her pain is particularly bad in her upper back and shoulders, and she notes morning stiffness. On examination, her joints are not inflamed, but she has symmetric "tender points" in the posterior neck, anterior chest, lateral buttocks, medial knees, and lateral elbows. You make a preliminary diagnosis of fibromyalgia.
Which one of the following diagnostic tests should you order?
A. Lyme titers
B. electromyelography
C. sedimentation rate
D. spine radiographs
E. screening test for depression
Correct Answer: C
Sleep disturbance is a characteristic symptom associated with fibromyalgia. Patients awaken feeling tired. The examination, other than tenderness in 14 specific, symmetrical points, is usually normal. Fever, rash on the extremities, muscle weakness, and migratory joint inflammation point to Lyme disease or other rheumatologic disorders. Asedimentation rate should be normal. If elevated, it may point to another diagnosis. Lyme titers are not indicated unless the patient has symptoms or history suggestive of the disease. Electromyelography and spine radiographs are typically normal and unnecessary for help in establishing the diagnosis. Depression can be associated with pain, but screening for it early on does not make sense and might offend the patient. Low-dose antidepressants often help to correct the sleep pattern and result in relief of pain. Nonsteroidal anti-inflammatory agents can also be used as needed; low-dose steroid is not indicated. Exercise is also helpful, and patients should be encouraged to stay physically active. Amoxicillin is not used for fibromyalgia. Benzodiazepines have addictive potential and lose their effectiveness for sleep after a few weeks.
Question 709:
A 35-year-old pharmacist complains of "hurting all over." Her pain is particularly bad in her upper back and shoulders, and she notes morning stiffness. On examination, her joints are not inflamed, but she has symmetric "tender points" in the posterior neck, anterior chest, lateral buttocks, medial knees, and lateral elbows. You make a preliminary diagnosis of fibromyalgia. Which of the following is another characteristic symptom associated with this syndrome?
A. sleep disturbance
B. fever
C. rash on the extremities
D. muscle weakness
E. migratory joint inflammation
Correct Answer: A
Sleep disturbance is a characteristic symptom associated with fibromyalgia. Patients awaken feeling tired. The examination, other than tenderness in 14 specific, symmetrical points, is usually normal. Fever, rash on the extremities, muscle weakness, and migratory joint inflammation point to Lyme disease or other rheumatologic disorders. Asedimentation rate should be normal. If elevated, it may point to another diagnosis. Lyme titers are not indicated unless the patient has symptoms or history suggestive of the disease. Electromyelography and spine radiographs are typically normal and unnecessary for help in establishing the diagnosis. Depression can be associated with pain, but screening for it early on does not make sense and might offend the patient. Low-dose antidepressants often help to correct the sleep pattern and result in relief of pain. Nonsteroidal anti-inflammatory agents can also be used as needed; low-dose steroid is not indicated. Exercise is also helpful, and patients should be encouraged to stay physically active. Amoxicillin is not used for fibromyalgia. Benzodiazepines have addictive potential and lose their effectiveness for sleep after a few weeks.
Question 710:
A 44-year-old man undergoes evaluation for worsening headaches. His posteroanterior and lateral arteriograms are shown in the figure below.Which of the following is the patient most likely to develop?
A. hypopituitarism
B. subarachnoid hemorrhage
C. hypercalcemia
D. tentorial herniation
E. chronic meningitis
Correct Answer: B
The arteriograms in figure demonstrate a large aneurysm arising from the basilar artery. Intracranial aneurysms occasionally present with new onset or worsening of headaches or may be asymptomatic and found coincidentally during evaluation of an unrelated disorder. Frequently, they leak or rupture, resulting in a subarachnoid hemorrhage with sudden onset of severe headache and meningeal symptoms and signs (e.g., nuchal rigidity, photophobia). Rapid progression to stroke, coma, or death may follow. Intracranial aneurysms are not usually associated with hypercalcemia, hypopituitarism, or chronic meningitis and rarely cause tentorial herniation without rupturing. Surgical approaches to intracranial aneurysms include excision and ligation.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.