In a 6-month-old previously healthy male infant, an abnormality is revealed during a routine diaper change, as illustrated in Figure. The parents have noted this finding on and off on several occasions over the last month. On each occasion, the child has been feeding well, and is content and playful.
Which of the following is the most appropriate management at this time?
A. antibiotics
B. reassurance to the parents that the abnormality will resolve without intervention
C. referral to the emergency department for immediate surgical consultation
D. referral for elective surgical repair
E. scrotal support
Correct Answer: D
This patient has an inguinoscrotal mass from an indirect inguinal hernia. His initial presentation is one of a reducible inguinal hernia. Repair is indicated because of the risk of incarceration. He should be referred for early elective surgery. The second presentation several weeks later is at the time of incarceration of the hernia. This has resulted in pain, irritability, and reflex vomiting. Prolonged incarceration increases the risk of bowel ischemia. The appropriate management is sedation with manual reduction, admission with observation in hospital, and surgical repair within 2448 hours. Delaying repair after an initial episode of incarceration increases the risk of further episodes of incarceration, with potential bowel or testicular compromise. Failure to reduce an incarcerated hernia successfully mandates urgent surgical intervention. Testicular torsion is uncommon in this age group and presents with a tender, high-riding testicle. When suspected, urgent surgical exploration is indicated. Inguinal adenitis may be the result of an inflammatory focus in the diaper area, with resultant adenopathy, and secondary infection of the inguinal nodes with a gram-positive organism. The infant is usually febrile, with a tender inguinal mass. Therapy includes systemic antibiotics. An undescended testicle may present as an inguinal mass, with an empty hemiscrotum. It is usually asymptomatic. Management is elective orchiopexy at approximately 1 year of age. A noncommunicating hydrocele presents as an asymptomatic, fluctuant scrotal mass that transilluminates. Surgical intervention is not required, because most will resolve spontaneously by 1 year of age
Question 82:
In a 6-month-old previously healthy male infant, an abnormality is revealed during a routine diaper change, as illustrated in Figure. The parents have noted this finding on and off on several occasions over the last month. On each occasion, the child has been feeding well, and is content and playful.
Which of the following is the most likely diagnosis?
A. noncommunicating hydrocele
B. inguinal adenitis
C. reducible inguinal hernia
D. incarcerated inguinal hernia
E. undescended testes
Correct Answer: C
This patient has an inguinoscrotal mass from an indirect inguinal hernia. His initial presentation is one of a reducible inguinal hernia. Repair is indicated because of the risk of incarceration. He should be referred for early elective surgery. The second presentation several weeks later is at the time of incarceration of the hernia. This has resulted in pain, irritability, and reflex vomiting. Prolonged incarceration increases the risk of bowel ischemia. The appropriate management is sedation with manual reduction, admission with observation in hospital, and surgical repair within 2448 hours. Delaying repair after an initial episode of incarceration increases the risk of further episodes of incarceration, with potential bowel or testicular compromise. Failure to reduce an incarcerated hernia successfully mandates urgent surgical intervention. Testicular torsion is uncommon in this age group and presents with a tender, high-riding testicle. When suspected, urgent surgical exploration is indicated. Inguinal adenitis may be the result of an inflammatory focus in the diaper area, with resultant adenopathy, and secondary infection of the inguinal nodes with a gram-positive organism. The infant is usually febrile, with a tender inguinal mass. Therapy includes systemic antibiotics. An undescended testicle may present as an inguinal mass, with an empty hemiscrotum. It is usually asymptomatic. Management is elective orchiopexy at approximately 1 year of age. A noncommunicating hydrocele presents as an asymptomatic, fluctuant scrotal mass that transilluminates. Surgical intervention is not required, because most will resolve spontaneously by 1 year of age
Question 83:
A 28-year-old man with a past history of bilateral orchiopexy for cryptorchidism presents with a painless, unilateral right scrotal enlargement. On examination, there is a palpable right testicular mass and enlarged inguinal nodes. Scrotal ultrasonography demonstrates heterogeneity of the testis, with an associated hydrocele. A CT scan of the abdomen and pelvis demonstrated right-sided retroperitoneal adenopathy. CT scan of the chest is normal.
Staging workup and surgery reveal a seminoma of the testicle, with positive inguinal and retroperitoneal nodes. Therapeutic management for this patient is which of the following?
A. external beam radiotherapy
B. multidrug combination chemotherapy
C. combination radiotherapy and multidrug chemotherapy
D. clinical surveillance
E. laparotomy with pelvic and retroperitoneal node dissection
Correct Answer: C
Cryptorchidism increases the risk of developing a testicular malignancy. This patient has a solid testicular mass which should be presumed to be secondary to a testicular malignancy. Optimal surgical management is inguinal exploration, control of the spermatic cord, biopsy of the mass, and radical orchiectomy with high ligation of the cord, if tumor is confirmed. Transscrotal aspiration, exploration, or needle biopsy is contraindicated because of risk of tumor spillage, and risk of altering the lymphatic drainage of the scrotum. Laparotomy and retroperitoneal node dissection is not indicated until after confirmation of the diagnosis and excision of the primary tumor. This patient has seminoma with disease spread to ipsilateral regional lymph nodes
Question 84:
A 28-year-old man with a past history of bilateral orchiopexy for cryptorchidism presents with a painless,
unilateral right scrotal enlargement. On examination, there is a palpable right testicular mass and enlarged
inguinal nodes. Scrotal ultrasonography demonstrates heterogeneity of the testis, with an associated
hydrocele. A CT scan of the abdomen and pelvis demonstrated right-sided retroperitoneal adenopathy. CT
scan of the chest is normal.
Which of the following would help confirm the diagnosis?
A. transscrotal needle biopsy
B. transscrotal aspiration of the hydrocele for cytology
C. radical orchiectomy through an inguinal incision
D. transscrotal exploration and orchiectomy
E. laparotomy with pelvic and retroperitoneal node dissection
Correct Answer: C
Cryptorchidism increases the risk of developing a testicular malignancy. This patient has a solid testicular mass which should be presumed to be secondary to a testicular malignancy. Optimal surgical management is inguinal exploration, control of the spermatic cord, biopsy of the mass, and radical orchiectomy with high ligation of the cord, if tumor is confirmed. Transscrotal aspiration, exploration, or needle biopsy is contraindicated because of risk of tumor spillage, and risk of altering the lymphatic drainage of the scrotum. Laparotomy and retroperitoneal node dissection is not indicated until after confirmation of the diagnosis and excision of the primary tumor. This patient has seminoma with disease spread to ipsilateral regional lymph nodes.
Question 85:
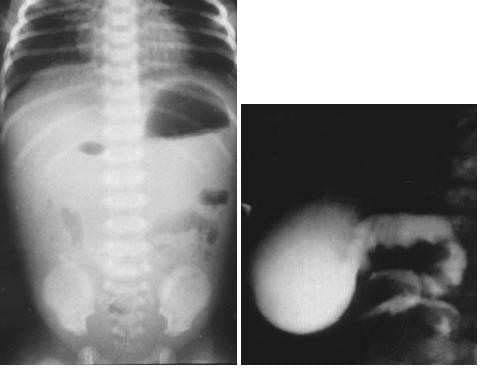
For each newborn with vomiting and illustrated radiographs, select the most likely diagnosis. A1-day- old infant with Down syndrome, feeding intolerance, bilious vomiting, and a double bubble on plain radiographs
A. congenital hypertrophic pyloric stenosis
B. annular pancreas
C. duodenal atresia
D. midgut volvulus
E. intussusception
F. imperforate anus
G. Meckel's diverticulum
H. meconium ileus
I. Hirschsprung's disease
J. jejunal atresia
Correct Answer: C
Pyloric stenosis presents with nonbilious vomiting and gastric distention. An annular pancreas does not result in obstruction, except when it is associated with an underlying duodenal abnormality. Duodenal atresia is associated with Down syndrome. It results in early onset of bilious vomiting from complete duodenal obstruction distal to the ampulla. There is a "double bubble" sign on plain abdominal radiographs from air in the stomach and proximal duodenum. Midgut volvulus is a life-threatening complication of malrotation. It presents with acute onset of bilious vomiting, usually in infants in the first year of life. There is a paucity of gas on plain radiographs, with evidence of duodenal obstruction. UGI contrast study will confirm the abnormal position of the duodenaljejunal junction and may demonstrate a corkscrew of the duodenum from volvulus. Intussusception is uncommon in newborns. Bilious vomiting is unusual at the outset, but may develop if the intussusception has been present for a significant time. Imperforate anus can be excluded by clinical examination.
If unrecognized, the infant will develop a clinical picture of a distal bowel obstruction, with dilated small and large bowel. Meckel's diverticulum can present with obstruction secondary to volvulus around a Meckel's band, with a distal small-bowel obstruction. Contrast enema will demonstrate a normal-caliber decompressed colon, with proximal dilated small bowel. Meconium ileus is associated with cystic fibrosis. Obstruction occurs from inspissated meconium in the terminal ileum. Plain radiographs may demonstrate a "soap bubble" pattern in the right lower quadrant, with a decompressed colon on contrast enema. Hirsch-sprung's disease presents with a distal bowel obstruction and delayed passage of meconium. A contrast enema may demonstrate a transition zone, with a narrow distal aganglionic segment, and proximal colonic dilatation. Jejunal atresia is a result of an intrauterine vascular accident. Infants present with bile- stained vomiting and abdominal distention early after birth. The colon is unused, and characteristically, on contrast enema, it is abnormally small in caliber
Question 86:
For each newborn with vomiting and illustrated radiographs, select the most likely diagnosis. Aneonate with bile-stained vomiting, abdominal distention, dilated loops of bowel on plain radiographs, and a small-caliber colon on contrast enema
A. congenital hypertrophic pyloric stenosis
B. annular pancreas
C. duodenal atresia
D. midgut volvulus
E. intussusception
F. imperforate anus
G. Meckel's diverticulum
H. meconium ileus
I. Hirschsprung's disease
J. jejunal atresia
Correct Answer: J
Pyloric stenosis presents with nonbilious vomiting and gastric distention. An annular pancreas does not result in obstruction, except when it is associated with an underlying duodenal abnormality. Duodenal atresia is associated with Down syndrome. It results in early onset of bilious vomiting from complete duodenal obstruction distal to the ampulla. There is a "double bubble" sign on plain abdominal radiographs from air in the stomach and proximal duodenum. Midgut volvulus is a life-threatening complication of malrotation. It presents with acute onset of bilious vomiting, usually in infants in the first year of life. There is a paucity of gas on plain radiographs, with evidence of duodenal obstruction. UGI contrast study will confirm the abnormal position of the duodenaljejunal junction and may demonstrate a corkscrew of the duodenum from volvulus. Intussusception is uncommon in newborns. Bilious vomiting is unusual at the outset, but may develop if the intussusception has been present for a significant time. Imperforate anus can be excluded by clinical examination.
If unrecognized, the infant will develop a clinical picture of a distal bowel obstruction, with dilated small and large bowel. Meckel's diverticulum can present with obstruction secondary to volvulus around a Meckel's band, with a distal small-bowel obstruction. Contrast enema will demonstrate a normal-caliber decompressed colon, with proximal dilated small bowel. Meconium ileus is associated with cystic fibrosis. Obstruction occurs from inspissated meconium in the terminal ileum. Plain radiographs may demonstrate a "soap bubble" pattern in the right lower quadrant, with a decompressed colon on contrast enema. Hirsch-sprung's disease presents with a distal bowel obstruction and delayed passage of meconium. A contrast enema may demonstrate a transition zone, with a narrow distal aganglionic segment, and proximal colonic dilatation. Jejunal atresia is a result of an intrauterine vascular accident. Infants present with bile- stained vomiting and abdominal distention early after birth. The colon is unused, and characteristically, on contrast enema, it is abnormally small in caliber
Question 87:
For each newborn with vomiting and illustrated radiographs, select the most likely diagnosis. A 10- day-old infant presenting with bilious vomiting, paucity of gas on plain radiographs, and duodenal obstruction on UGI contrast study
A. congenital hypertrophic pyloric stenosis
B. annular pancreas
C. duodenal atresia
D. midgut volvulus
E. intussusception
F. imperforate anus
G. Meckel's diverticulum
H. meconium ileus
I. Hirschsprung's disease
J. jejunal atresia
Correct Answer: D
Pyloric stenosis presents with nonbilious vomiting and gastric distention. An annular pancreas does not result in obstruction, except when it is associated with an underlying duodenal abnormality. Duodenal atresia is associated with Down syndrome. It results in early onset of bilious vomiting from complete duodenal obstruction distal to the ampulla. There is a "double bubble" sign on plain abdominal radiographs from air in the stomach and proximal duodenum. Midgut volvulus is a life-threatening complication of malrotation. It presents with acute onset of bilious vomiting, usually in infants in the first year of life. There is a paucity of gas on plain radiographs, with evidence of duodenal obstruction. UGI contrast study will confirm the abnormal position of the duodenaljejunal junction and may demonstrate a corkscrew of the duodenum from volvulus. Intussusception is uncommon in newborns. Bilious vomiting is unusual at the outset, but may develop if the intussusception has been present for a significant time. Imperforate anus can be excluded by clinical examination.
If unrecognized, the infant will develop a clinical picture of a distal bowel obstruction, with dilated small and large bowel. Meckel's diverticulum can present with obstruction secondary to volvulus around a Meckel's band, with a distal small-bowel obstruction. Contrast enema will demonstrate a normal-caliber decompressed colon, with proximal dilated small bowel. Meconium ileus is associated with cystic fibrosis.
Obstruction occurs from inspissated meconium in the terminal ileum. Plain radiographs may demonstrate a "soap bubble" pattern in the right lower quadrant, with a decompressed colon on contrast enema. Hirsch-sprung's disease presents with a distal bowel obstruction and delayed passage of meconium. A contrast enema may demonstrate a transition zone, with a narrow distal aganglionic segment, and proximal colonic dilatation. Jejunal atresia is a result of an intrauterine vascular accident. Infants present with bile- stained vomiting and abdominal distention early after birth. The colon is unused, and characteristically, on contrast enema, it is abnormally small in caliber
Question 88:
A 35-year-old woman is involved in a motor vehicle crash, sustaining a severe pelvic fracture, with disruption of the pelvic ring. In the trauma resuscitation room, she is confused and tachypneic, with a blood pressure of 90 mmHg systolic and a heart rate of 130/min. Laboratory investigations include serum electrolyte analysis, revealing a sodium of 139, a chloride of 103, and a bicarbonate of 14 meq/L. Which of the following is the most appropriate management of this acid-based derangement?
A. administration of sodium bicarbonate to correct the base deficit
B. restoration of blood volume with aggressive IV fluid resuscitation
C. IV hydrochloric acid
D. intubation and hyperventilation
E. this patient has no acid-based abnor
Correct Answer: B
This patient is acidotic, with a low serum bicarbonate (bicarbonate depletion defined as a serum bicarbonate less than 22 meq/L). She has hypovolemic shock from trauma and acute blood loss, resulting in decreased tissue perfusion and lactic acidosis. The resultant elevated anion gap (139 - [103 + 14] = 22 meq/L with a normal anion gap of 816 meq/L) is from the increased lactic acid. The tachypnea may be caused by the respiratory compensation with decreased PCO2. Correction of the acidosis should be aimed at improving tissue perfusion with aggressive IV fluid resuscitation. Metabolic alkalosis is associated with serum bicarbonate greater than 26 meq/L. Respiratory acidosis is related to primary carbon dioxide retention from decreased alveolar ventilation. Administration of sodium bicarbonate is indicated only in severe acidosis (pH <7.2), and in patients with evidence of myocardial instability or arrhythmias. Hydrochloric acid is indicated only in life-threatening metabolic alkalosis that is not chloride responsive. Respiratory acidosis with alveolar hypoventilation may be corrected with assisted ventilation
Question 89:
A 35-year-old woman is involved in a motor vehicle crash, sustaining a severe pelvic fracture, with disruption of the pelvic ring. In the trauma resuscitation room, she is confused and tachypneic, with a blood pressure of 90 mmHg systolic and a heart rate of 130/min. Laboratory investigations include serum electrolyte analysis, revealing a sodium of 139, a chloride of 103, and a bicarbonate of 14 meq/L. This patient demonstrates which of the following?
A. nonanion gap metabolic acidosis
B. anion gap metabolic acidosis
C. metabolic alkalosis
D. respiratory acidosis
E. normal serum electrolytes
Correct Answer: B
This patient is acidotic, with a low serum bicarbonate (bicarbonate depletion defined as a serum bicarbonate less than 22 meq/L). She has hypovolemic shock from trauma and acute blood loss, resulting in decreased tissue perfusion and lactic acidosis. The resultant elevated anion gap (139 - [103 + 14] = 22 meq/L with a normal anion gap of 816 meq/L) is from the increased lactic acid. The tachypnea may be caused by the respiratory compensation with decreased PCO2. Correction of the acidosis should be aimed at improving tissue perfusion with aggressive IV fluid resuscitation. Metabolic alkalosis is associated with serum bicarbonate greater than 26 meq/L. Respiratory acidosis is related to primary carbon dioxide retention from decreased alveolar ventilation. Administration of sodium bicarbonate is indicated only in severe acidosis (pH <7.2), and in patients with evidence of myocardial instability or arrhythmias. Hydrochloric acid is indicated only in life-threatening metabolic alkalosis that is not chloride responsive. Respiratory acidosis with alveolar hypoventilation may be corrected with assisted ventilation
Question 90:
A 6-year-old boy presents to the emergency department with a painful, markedly swollen elbow. While ice-skating, he fell with his arm outstretched. Radiographs of the elbow demonstrate a displaced, supracondylar fracture of the humerus. On examination, there is pain on passive flexion at the wrist and a decreased radial pulse, with diminished capillary refill in the hand. Which of the following is the most appropriate management of this injury?
A. admission to hospital for close observation, with immobilization of the elbow at 90皁f flexion
B. closed reduction with percutaneous pinning under general anesthesia
C. open reduction and pinning under general anesthesia
D. open reduction with pinning, and exploration of the brachial artery
E. open reduction with pinning, exploration of the brachial artery, and decompression fasciotomy of the forearm fascial compartments
Correct Answer: E
This child has a displaced supracondylar fracture associated with vascular compromise of the forearm from associated brachial artery compression, distortion, or vessel injury. Decreased perfusion below the fracture in conjunction with pain on passive wrist flexion are signs of a developing forearm compartment syndrome. Management should include operative exploration of the brachial artery, open reduction and pinning of the fracture, and forearm compartment fasciotomy to limit progression of muscular ischemia. Immobilization of the elbow at 90癷s suitable only for undisplaced f ractures. For displaced fractures without neurovascular compromise, closed reduction and pinning may be adequate, but if adequate reduction cannot be achieved, open reduction may be required.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.