Mr. Jones is a 34-year-old married businessman. He and his wife are both patients in your practice. As part of his annual physical, you screen for high-risk behaviors and he admits to receiving confidential treatment at a public health clinic for gonorrhea and genital herpes. He has not revealed this information to his wife even though they are planning to have a baby. He did not return for the results of HIV screening at the public health clinic. On physical examination, you note that he has cervical and axillary lymphadenopathy, oral thrush, and seborrheic dermatitis. What is the best step in his clinical management?
A. Prescribe Mycelex troches.
B. Schedule a lymph node biopsy.
C. Prescribe Lotrisone (betamethasone/clotrimazole) cream.
D. Repeat HIV serologic testing.
E. Contact his wife for sexually transmitted disease (STD) screening.
Correct Answer: D Section: (none)
Explanation:
Although Mycelex troches would be appropriate in the management of his oral candidiasis and the Lotrisone would treat his seborrheic dermatitis, the patient has previously described risk factors for HIV infection and physical symptoms of immunodeficiency. Accurate knowledge of his HIV status is essential in the appropriate long-term management of this patient. In fact, his current physical examination suggests long-standing HIV infection. A lymph node biopsy is not warranted. His wife will eventually need screening for STDs since active STDs increase her risk of cotransmission of HIV. The patient's refusal to discuss his situation with his wife raises many controversial issues with no simple solution. There are multiple arguments which support the ethical guidelines for supporting patient confidentiality. These include: · An appeal to consequences (potential patient discrimination secondary to health information; importance of trust) · Appeal to virtue (physician fidelity) · Respect (awareness and compassion for patient vulnerability) · Do no harm (breach of medical information may lead to discrimination) Respect for patient autonomy incorporates the patient in the treatment process and is based on mutual trust. Referring Mr. Jones to another physician doesn't address the concerns involved in the care of Mrs. Jones. The Tarasoff case (1976) established the following precedent: Patient confidentiality must be upheld as part of the protected clinicianpatient relationship but the physician has a duty to warn specific, innocent third parties of potential harm threatened or posed by the patient. In fact, failure to warn by the physician may constitute negligence. This is not the law in all states. Some states interpret the standard as a strict duty to warn; other states permit physicians to warn affected third parties but not require it. If the physician unilaterally discloses the HIV status, it would represent a breach of confidentiality. However, their marital status may allow this disclosure. Even if the patient is adamant in his refusal, the physician needs to determine the reasons for his reticence. As his physician, you can provide additional information about HIV prevention and treatment. It would be highly unusual for Mr. Jones to ultimately refuse notification of his spouse once he has been urged to do so by his physician. The mechanism for how these complex issues are addressed has potential ramifications for his future trust of physicians, consent to HAART (highly active antiretroviral therapy) treatment, and medication compliance. If these barriers to disclosure cannot be addressed within the physician-patient relationship, the health department can provide a mechanism for contact testing. Although you could ask Mrs. Jones to come in for a physical examination, she might refuse to have STD tests performed, especially if she perceives herself to be at minimal risk. Ideally, this assessment should be performed prior to a pregnancy. If she is currently HIV negative, then protective measures against future infection can be introduced.
Question 122:
The modern history of the protection of human research subjects began in the twentieth century in response to human experimentation which occurred during World War II. The Nuremberg Military Tribunal set forth initial basic standards for the conduct of research which ultimately became known as the Nuremberg Code (1947/1948). In subsequent years, these recommendations have been modified and expanded to reflect various aspects of medical ethics in biomedical and behavioral research. These international ethical guidelines include the Declaration of Helsinki (1964), the Belmont Report (1979), CIOMS (1982), and the Common Rule (1991). The concept of justice as described in the Belmont Report means which of the following?
A. ensuring that risks to research subjects are minimized
B. ensuring the protection of privacy
C. maintaining confidentiality
D. ensuring informed consent
E. ensuring the equitable distribution of research burdens and benefits
Correct Answer: E Section: (none)
Explanation:
On September 30, 1978, the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research submitted the report "Ethical Principles and Guidelines for the Protection of Human Subjects of Research," named after the Belmont Conference Center in the Smithsonian Institution. The three ethical principles emphasized in this report include justice, beneficence, and respect for persons. Justice is the equitable distribution of research burdens and benefits. Beneficence is the mechanism to maximize benefits and minimize harm to research subjects. Respect for persons is the ethical principle which prioritizes the respect for individual autonomy and the protection of individuals with reduced autonomy. The principle of respect emphasizes the protection of subjects' privacy, maintenance of confidentiality, informed consent, and the utilization of additional safeguards for the protection of vulnerable populations. Health and Human Service (HHS) regulations delineate additional mechanisms to protect human subjects, which include (1) institutional assurances of compliance, (2) Institutional Review Board (IRB) review, and
(3) informed consent. An institutional assurance of compliance is documentation that the institution will follow HHS regulations for the protection of human subjects. An IRB is a committee that has been established to protect human subjects involved in research activities. These committees must have at least five members of varying backgrounds who possess the professional competence to review research activities. Informed consent is the voluntary choice of an individual to participate in research activities. To be truly informed consent, the individual must have a clear and accurate understanding of the purpose of the research, the risks involved, the potential benefits, the procedures to be performed and the alternative modalities of treatment available. Typically, these are in a written consent form. The legal arguments for informed consent emphasize the right of self determination. This is in contrast to the ethical basis of individual autonomy. Therefore, a mere signature by the individual participant does not fulfill the ethical requirements of the informed consent process. Any research study must have scientific validity, a fair selection of individual subjects for populations, protection of vulnerable populations, fair access to the benefits of medical research, acceptable risk-benefit ratios, appropriate informed consent, and independent review of the study. In addition, Data Safety Monitoring Boards are being utilized to further monitor the safety of research protocols and participation.
Question 123:
The modern history of the protection of human research subjects began in the twentieth century in response to human experimentation which occurred during World War II. The Nuremberg Military Tribunal set forth initial basic standards for the conduct of research which ultimately became known as the Nuremberg Code (1947/1948). In subsequent years, these recommendations have been modified and expanded to reflect various aspects of medical ethics in biomedical and behavioral research. These
international ethical guidelines include the Declaration of Helsinki (1964), the Belmont Report (1979),
CIOMS (1982), and the Common Rule (1991).
The concept of beneficence in the Belmont Report emphasizes the importance of which of the following?
A. establishing institutional research boards (IRBs)
B. maximizing benefits and minimizing harms to research subjects
C. ensuring independent ethical review of research
D. ensuring scientific validity of research
E. including patient advocates on scientific advisory boards
Correct Answer: B Section: (none)
Explanation:
On September 30, 1978, the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research submitted the report "Ethical Principles and Guidelines for the Protection of Human Subjects of Research," named after the Belmont Conference Center in the Smithsonian Institution. The three ethical principles emphasized in this report include justice, beneficence, and respect for persons. Justice is the equitable distribution of research burdens and benefits. Beneficence is the mechanism to maximize benefits and minimize harm to research subjects. Respect for persons is the ethical principle which prioritizes the respect for individual autonomy and the protection of individuals with reduced autonomy. The principle of respect emphasizes the protection of subjects' privacy, maintenance of confidentiality, informed consent, and the utilization of additional safeguards for the protection of vulnerable populations. Health and Human Service (HHS) regulations delineate additional mechanisms to protect human subjects, which include (1) institutional assurances of compliance, (2) Institutional Review Board (IRB) review, and
(3) informed consent. An institutional assurance of compliance is documentation that the institution will follow HHS regulations for the protection of human subjects. An IRB is a committee that has been established to protect human subjects involved in research activities. These committees must have at least five members of varying backgrounds who possess the professional competence to review research activities. Informed consent is the voluntary choice of an individual to participate in research activities. To be truly informed consent, the individual must have a clear and accurate understanding of the purpose of the research, the risks involved, the potential benefits, the procedures to be performed and the alternative modalities of treatment available. Typically, these are in a written consent form. The legal arguments for informed consent emphasize the right of self determination. This is in contrast to the ethical basis of individual autonomy. Therefore, a mere signature by the individual participant does not fulfill the ethical requirements of the informed consent process. Any research study must have scientific validity, a fair selection of individual subjects for populations, protection of vulnerable populations, fair access to the benefits of medical research, acceptable risk-benefit ratios, appropriate informed consent, and independent review of the study. In addition, Data Safety Monitoring Boards are being utilized to further monitor the safety of research protocols and participation.
Question 124:
A 1-year-old boy is brought to the office for a well-child examination. Your office nurse has plotted his growth on the following chart (see Figure 6-1). The most appropriate initial management of this abnormality is which of the following?
A. Order a CT scan of the head.
B. Repeat the measurement.
C. Recommend that the mother cut down on the child's caloric intake.
D. Review the growth chart of the child's older sibling to look for a similar pattern.
E. Ask the mother to bring the child back to the office at monthly intervals to follow his growth more closely.
Correct Answer: B Section: (none)
Explanation:
The most common reason for an unusual or unexpected finding on a pediatric growth chart is erroneous measurement. Whenever such an occurrence is noted, the first intervention should be to repeat and confirm the measurement. All of the other options may be appropriate for further evaluation and management if the abnormality noted is confirmed to be real.
Question 125:
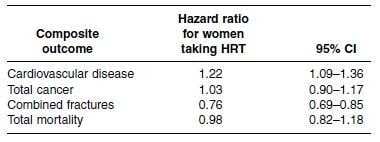
A 60-year-old woman presents to your office to discuss her ongoing treatment with HRT that she takes for menopausal symptoms. She was started on estrogen and progesterone replacement at the age of 51 and has been on them since that time. She has read several articles in newspapers and on the Internet stating that hormone therapy is dangerous. You briefly review the results of the Women's Health Initiative study, a randomized-controlled trial comparing health outcomes in women taking combined estrogen-progestin therapy (HRT) versus a placebo. The results are as follows:
The authors provided composite data on total cardiovascular disease, cancer, fracture, and mortality risks, which are summarized in the chart.
Based on the data presented, which of the following statements is true?
A. There is an increase in total cancer risk for women on HRT.
B. There is an increase in cardiovascular disease risk for women on HRT.
C. There is an increase in combined fracture risk for women on HRT.
D. There is a reduction in total mortality for women on HRT.
E. There is an overall detriment to the quality of life of women on HRT.
Correct Answer: B Section: (none)
Explanation:
The hazard ratio statistic as presented is a comparison of the rate of development of an outcome in the treatment group divided by the rate of development of the same outcome in the control group. It is a "hazard" ratio because all of the outcomes measured are adverse. Ahazard ratio of 1.00 means that there is no difference in the rate of development of the outcome between the two groups. Further, if the 95% CI crosses 1.00 then there is no statistically significant difference between the two groups. From the data presented, the hazard ratio for the development of endometrial cancer is 0.83, suggesting that there may be a reduction in the risk of endometrial cancer for women on HRT. However, the 95% CI crosses 1, therefore we cannot consider this result to be statistically significant. For the other outcomes listed, the 95% CIs do not cross 1.00, thus representing statistically significant increases in the risk of CHD, pulmonary embolism, and stroke and a statistically significant reduction in the risk of hip fracture. In question 69, the data reveal statistically significant rates of combined cardiovascular disease and fracture risk between the two groups. The risk of cardiovascular disease is increased but the combined fracture risk is reduced in women on HRT. The combined cancer risk and total mortality do not reach the level of statistical significance. There are no data presented on quality of life in the chart, so we cannot state that option E is true.
Question 126:
A 60-year-old woman presents to your office to discuss her ongoing treatment with HRT that she takes for menopausal symptoms. She was started on estrogen and progesterone replacement at the age of 51 and has been on them since that time. She has read several articles in newspapers and on the Internet stating that hormone therapy is dangerous. You briefly review the results of the Women's Health Initiative study, a randomized-controlled trial comparing health outcomes in women taking combined estrogen-progestin therapy (HRT) versus a placebo. The results are as follows:
Based on the results listed, what can you tell your patient about women taking HRT?
A. They have no difference in endometrial cancer risk.
B. They have no difference in CHD risk.
C. They have no difference in pulmonary embolus risk.
D. They have no difference in stroke risk.
E. They have no difference in hip fracture risk.
Correct Answer: A Section: (none)
Explanation:
The hazard ratio statistic as presented is a comparison of the rate of development of an outcome in the treatment group divided by the rate of development of the same outcome in the control group. It is a "hazard" ratio because all of the outcomes measured are adverse. Ahazard ratio of 1.00 means that there is no difference in the rate of development of the outcome between the two groups. Further, if the 95% CI crosses 1.00 then there is no statistically significant difference between the two groups. From the data presented, the hazard ratio for the development of endometrial cancer is 0.83, suggesting that there may be a reduction in the risk of endometrial cancer for women on HRT. However, the 95% CI crosses 1, therefore we cannot consider this result to be statistically significant. For the other outcomes listed, the 95% CIs do not cross 1.00, thus representing statistically significant increases in the risk of CHD, pulmonary embolism, and stroke and a statistically significant reduction in the risk of hip fracture. In question 69, the data reveal statistically significant rates of combined cardiovascular disease and fracture risk between the two groups. The risk of cardiovascular disease is increased but the combined fracture risk is reduced in women on HRT. The combined cancer risk and total mortality do not reach the level of statistical significance. There are no data presented on quality of life in the chart, so we cannot state that option E is true.
Question 127:
A 49-year-old male postal worker presents to your office for the evaluation of a lesion on his left arm. The lesion started about a week ago as a red pustule but has grown and now has a thick black scab. The lesion is painless. A coworker showed the patient a similar appearing lesion that she developed on her arm for which her doctor prescribed an oral antibiotic. Examination reveals a 5 cm circular black eschar with some surrounding vesicles. A Gram stain of fluid drained from a vesicle reveals chains of gram-positive bacilli. Which of the following is characteristic of Varicella (chickenpox) but not smallpox?
A. The mortality rate is high.
B. The lesions are commonly on the palms of the hands and soles of the feet.
C. The pox lesions evolve synchronously.
D. There is typically a 2-to 4-day prodrome of fever, malaise, headache, and backache before the development of the rash.
E. The vesicles typically occur on an erythematous base (described as dewdrops on a rose petal)
Correct Answer: E Section: (none)
Explanation:
B. anthracis causes three diseases in humans: cutaneous, inhalation, and gastrointestinal anthrax. Cutaneous anthrax is the most common of the naturally occurring anthrax diseases. The spores of the gram-positive bacillus can survive for years in soil. The disease cutaneous anthrax occurs when the spores contaminate a wound on the skin of the victim and then start to grow. This disease occurs most commonly in agricultural areas where the soil becomes contaminated by the presence of animals. Initially a painless papule develops, followed by vesicles which then ulcerate and a black eschar forms. In the setting of cutaneous anthrax in a postal worker who has a coworker with an apparently similar disease, bioterrorism must be suspected. This type of attack occurred in the Fall of 2001, when anthrax spores were sent through the U.S. Postal system and over 20 persons were infected. In this setting, the most appropriate initial management is to immediately contact the appropriate Public Health Authorities, usually the local or state health department. Appropriate treatment will also need to be instituted, under the guidance of the public health specialists, as untreated cutaneous anthrax may carry a 20% mortality rate. Antibiotic therapy would usually be with ciprofloxacin, penicillin, or doxycycline. Anthrax does not spread from person to person, so quarantine is not necessary. Inhalation anthrax is caused by the direct inhalation of spores into the lungs and gastrointestinal anthrax, the least common of the anthrax syndromes, is caused by ingestion. Smallpox does not occur naturally anywhere in the world. Therefore, any suspicion of smallpox must be assumed to be a bioterror event and must be reported immediately to public health officials. Physicians should be able to recognize the signs and symptoms of smallpox and be able to distinguish them from the common occurrence of chickenpox. Chickenpox lesions tend to occur in clusters and evolve asynchronously. They are often described as "dew drops on a rose petal" as they are vesicles occurring on an erythematous base. The lesions tend to start on the trunk and rapidly spread outward. The rash will be associated with a fever but there are usually few to no prodromal symptoms. Because of the asynchronous growth and outbreaks, a patient will typically have lesions in different stages of evolution. In contrast, smallpox lesions tend to occur synchronously and the lesions tend to be uniform. The rash frequently occurs on the palms and soles. It typically starts on the face and arms and then spreads to the trunk and legs. The development of the rash tends to be slower than that of chickenpox. There is often a dramatic prodrome of high fever, malaise, headache, and backache for 24 days prior to the onset of the rash. Smallpox carries an approximately 30% mortality, while mortality associated with chickenpox is very low.
Question 128:
A 49-year-old male postal worker presents to your office for the evaluation of a lesion on his left arm. The lesion started about a week ago as a red pustule but has grown and now has a thick black scab. The lesion is painless. A coworker showed the patient a similar appearing lesion that she developed on her arm for which her doctor prescribed an oral antibiotic. Examination reveals a 5 cm circular black eschar with some surrounding vesicles. A Gram stain of fluid drained from a vesicle reveals chains of gram-positive bacilli. The patient asks how he contracted this infection. Which of the following do you tell him?
A. from direct contact with the coworker who had the similar appearing lesion
B. ingestion of contaminated food in the postal facility cafeteria
C. a small skin cut or sore was directly contaminated with spores
D. inhalation of bacteria from a contaminated ventilation system
E. exposure to respiratory droplets from an infected person
Correct Answer: C Section: (none)
Explanation:
B. anthracis causes three diseases in humans: cutaneous, inhalation, and gastrointestinal anthrax. Cutaneous anthrax is the most common of the naturally occurring anthrax diseases. The spores of the gram-positive bacillus can survive for years in soil. The disease cutaneous anthrax occurs when the spores contaminate a wound on the skin of the victim and then start to grow. This disease occurs most commonly in agricultural areas where the soil becomes contaminated by the presence of animals. Initially a painless papule develops, followed by vesicles which then ulcerate and a black eschar forms. In the setting of cutaneous anthrax in a postal worker who has a coworker with an apparently similar disease, bioterrorism must be suspected. This type of attack occurred in the Fall of 2001, when anthrax spores were sent through the U.S. Postal system and over 20 persons were infected. In this setting, the most appropriate initial management is to immediately contact the appropriate Public Health Authorities, usually the local or state health department. Appropriate treatment will also need to be instituted, under the guidance of the public health specialists, as untreated cutaneous anthrax may carry a 20% mortality rate. Antibiotic therapy would usually be with ciprofloxacin, penicillin, or doxycycline. Anthrax does not spread from person to person, so quarantine is not necessary. Inhalation anthrax is caused by the direct inhalation of spores into the lungs and gastrointestinal anthrax, the least common of the anthrax syndromes, is caused by ingestion. Smallpox does not occur naturally anywhere in the world. Therefore, any suspicion of smallpox must be assumed to be a bioterror event and must be reported immediately to public health officials. Physicians should be able to recognize the signs and symptoms of smallpox and be able to distinguish them from the common occurrence of chickenpox. Chickenpox lesions tend to occur in clusters and evolve asynchronously. They are often described as "dew drops on a rose petal" as they are vesicles occurring on an erythematous base. The lesions tend to start on the trunk and rapidly spread outward. The rash will be associated with a fever but there are usually few to no prodromal symptoms. Because of the asynchronous growth and outbreaks, a patient will typically have lesions in different stages of evolution. In contrast, smallpox lesions tend to occur synchronously and the lesions tend to be uniform. The rash frequently occurs on the palms and soles. It typically starts on the face and arms and then spreads to the trunk and legs. The development of the rash tends to be slower than that of chickenpox. There is often a dramatic prodrome of high fever, malaise, headache, and backache for 24 days prior to the onset of the rash. Smallpox carries an approximately 30% mortality, while mortality associated with chickenpox is very low.
Question 129:
A 49-year-old male postal worker presents to your office for the evaluation of a lesion on his left arm. The lesion started about a week ago as a red pustule but has grown and now has a thick black scab. The lesion is painless. A coworker showed the patient a similar appearing lesion that she developed on her arm for which her doctor prescribed an oral antibiotic. Examination reveals a 5 cm circular black eschar with some surrounding vesicles. A Gram stain of fluid drained from a vesicle reveals chains of gram-positive bacilli. What is the most appropriate management at this point?
A. topical mupirocin ointment tid for 10 days
B. oral cephalexin 500 mg qid for a week
C. oral clindamycin 300 mg tid for 10 days
D. urgent quarantine of patient's coworkers and family contacts
E. immediate notification of Public Health Authorities
Correct Answer: E Section: (none)
Explanation:
B. anthracis causes three diseases in humans: cutaneous, inhalation, and gastrointestinal anthrax. Cutaneous anthrax is the most common of the naturally occurring anthrax diseases. The spores of the gram-positive bacillus can survive for years in soil. The disease cutaneous anthrax occurs when the spores contaminate a wound on the skin of the victim and then start to grow. This disease occurs most commonly in agricultural areas where the soil becomes contaminated by the presence of animals. Initially a painless papule develops, followed by vesicles which then ulcerate and a black eschar forms. In the setting of cutaneous anthrax in a postal worker who has a coworker with an apparently similar disease, bioterrorism must be suspected. This type of attack occurred in the Fall of 2001, when anthrax spores were sent through the U.S. Postal system and over 20 persons were infected. In this setting, the most appropriate initial management is to immediately contact the appropriate Public Health Authorities, usually the local or state health department. Appropriate treatment will also need to be instituted, under the guidance of the public health specialists, as untreated cutaneous anthrax may carry a 20% mortality rate. Antibiotic therapy would usually be with ciprofloxacin, penicillin, or doxycycline. Anthrax does not spread from person to person, so quarantine is not necessary. Inhalation anthrax is caused by the direct inhalation of spores into the lungs and gastrointestinal anthrax, the least common of the anthrax syndromes, is caused by ingestion. Smallpox does not occur naturally anywhere in the world. Therefore, any suspicion of smallpox must be assumed to be a bioterror event and must be reported immediately to public health officials. Physicians should be able to recognize the signs and symptoms of smallpox and be able to distinguish them from the common occurrence of chickenpox. Chickenpox lesions tend to occur in clusters and evolve asynchronously. They are often described as "dew drops on a rose petal" as they are vesicles occurring on an erythematous base. The lesions tend to start on the trunk and rapidly spread outward. The rash will be associated with a fever but there are usually few to no prodromal symptoms. Because of the asynchronous growth and outbreaks, a patient will typically have lesions in different stages of evolution. In contrast, smallpox lesions tend to occur synchronously and the lesions tend to be uniform. The rash frequently occurs on the palms and soles. It typically starts on the face and arms and then spreads to the trunk and legs. The development of the rash tends to be slower than that of chickenpox. There is often a dramatic prodrome of high fever, malaise, headache, and backache for 24 days prior to the onset of the rash. Smallpox carries an approximately 30% mortality, while mortality associated with chickenpox is very low.
Question 130:
A 49-year-old male postal worker presents to your office for the evaluation of a lesion on his left arm. The lesion started about a week ago as a red pustule but has grown and now has a thick black scab. The lesion is painless. A coworker showed the patient a similar appearing lesion that she developed on her arm for which her doctor prescribed an oral antibiotic. Examination reveals a 5 cm circular black eschar with some surrounding vesicles. A Gram stain of fluid drained from a vesicle reveals chains of gram-positive bacilli. What organism is most likely responsible for this lesion?
A. methicillin-resistant Staphylococcus aureus
B. smallpox virus
C. Clostridium tetani
D. Bacillus anthracis
E. group A beta-hemolytic Streptococcus
Correct Answer: D Section: (none)
Explanation:
B. anthracis causes three diseases in humans: cutaneous, inhalation, and gastrointestinal anthrax. Cutaneous anthrax is the most common of the naturally occurring anthrax diseases. The spores of the gram-positive bacillus can survive for years in soil. The disease cutaneous anthrax occurs when the spores contaminate a wound on the skin of the victim and then start to grow. This disease occurs most commonly in agricultural areas where the soil becomes contaminated by the presence of animals. Initially a painless papule develops, followed by vesicles which then ulcerate and a black eschar forms. In the setting of cutaneous anthrax in a postal worker who has a coworker with an apparently similar disease, bioterrorism must be suspected. This type of attack occurred in the Fall of 2001, when anthrax spores were sent through the U.S. Postal system and over 20 persons were infected. In this setting, the most appropriate initial management is to immediately contact the appropriate Public Health Authorities, usually the local or state health department. Appropriate treatment will also need to be instituted, under the guidance of the public health specialists, as untreated cutaneous anthrax may carry a 20% mortality rate. Antibiotic therapy would usually be with ciprofloxacin, penicillin, or doxycycline. Anthrax does not spread from person to person, so quarantine is not necessary. Inhalation anthrax is caused by the direct inhalation of spores into the lungs and gastrointestinal anthrax, the least common of the anthrax syndromes, is caused by ingestion. Smallpox does not occur naturally anywhere in the world. Therefore, any suspicion of smallpox must be assumed to be a bioterror event and must be reported immediately to public health officials. Physicians should be able to recognize the signs and symptoms of smallpox and be able to distinguish them from the common occurrence of chickenpox. Chickenpox lesions tend to occur in clusters and evolve asynchronously. They are often described as "dew drops on a rose petal" as they are vesicles occurring on an erythematous base. The lesions tend to start on the trunk and rapidly spread outward. The rash will be associated with a fever but there are usually few to no prodromal symptoms. Because of the asynchronous growth and outbreaks, a patient will typically have lesions in different stages of evolution. In contrast, smallpox lesions tend to occur synchronously and the lesions tend to be uniform. The rash frequently occurs on the palms and soles. It typically starts on the face and arms and then spreads to the trunk and legs. The development of the rash tends to be slower than that of chickenpox. There is often a dramatic prodrome of high fever, malaise, headache, and backache for 24 days prior to the onset of the rash. Smallpox carries an approximately 30% mortality, while mortality associated with chickenpox is very low.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.