A39-year-old woman with a long-standing history of normal pap smears undergoes a total abdominal hysterectomy for a large uterine fibroid and menorrhagia. Six months after her hysterectomy she had a negative vaginal pap smear from the vaginal apex. She presents to your clinic today for a routine physical examination. Based on the American College of Obstetricians and Gynecologists recommendations, when should this patient have pap smears?
A. yearly
B. every 3 years
C. every 5 years
D. never again
E. only if she develops risk factors
Correct Answer: E Section: (none)
Explanation:
This patient, who had a hysterectomy for a benign condition, no longer needs pap smear screening as long as she is monogamous and does not develop risk factors for cervical dysplasia. The incidence for vaginal dysplasia after hysterectomy for benign disease is approximately 0.13%. Invasive carcinoma of the vagina is rare, and screening for this cancer is not cost-effective. However, women who had a hysterectomy for cervical dysplasia or cancer are at increased risk for vaginal dysplasia and should continue to have vaginal pap smears. It is also reasonable to reinitiate pap smear screening in women who had a hysterectomy for benign disease if they have new sexual partners or new risk factors. Apap test is also indicated if patients present with vaginal spotting or bleeding
Question 352:
A22-year-old nulliparous woman who desires future fertility is found to have a pap smear consistent with high-grade squamous intraepithelial lesion (HGSIL). The final pathology report indicates a single focus of squamous carcinoma invasive into the cervical stroma to a depth of 2.0 mm. An ECC is negative. There is no lymphvascular space invasion, and the cone margins are negative. The most appropriate therapy for this patient is which of the following?
A. radiation therapy
B. simple hysterectomy with pelvic lymphadenectomy
C. radical hysterectomy with pelvic lymphadenectomy
D. radical trachelectomy
E. observation with close follow-up
Correct Answer: E Section: (none)
Explanation:
Current American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines for treating a pap smear consistent with HGSIL is to perform colposcopy with directed biopsies if a lesion is seen. Routine pap smear in 1 year is an unacceptable option for this patient given her increased risk for developing cervical cancer. Random biopsies have a high false negative rate if there is no visible lesion to biopsy, thus, are not helpful. The pap smear is a screening test of the cervix, not the endometrium. There is no reason to suspect that this patient has endometrial pathology, therefore, an endometrial biopsy is not warranted. HPV testing is not recommended for high-grade pap smears. All high-grade pap smears require further investigation with colposcopy regardless of HPV status. If colposcopy is unsatisfactory, meaning no lesion is identified, the full transformation zone is not visualized or the full extent of the lesion is not identified, then a diagnostic excisional procedure is warranted. A loop excisional electrocautery procedure (LEEP) would be appropriate. However, note that if your suspicion for cancer is high, the cauterized edges from a LEEP procedure can complicate the pathologic assessment of positive margins. A cold knife cervical conization can be performed in the operating room as an outpatient surgery and provides the best surgical specimen for pathologic evaluation. In this case, a TVUS, endometrial dilation, and curettage, and ECC are all inappropriate options since they do not accurately evaluate the cervix, which is the primary site of concern. This patient has, by definition, microinvasive cervical cancer. Approximately 1015% of patients in the United States with stage I cervical cancer will have a microinvasive cancer. Microinvasive cancer is defined as stage IA with invasion limited to a depth of 5 mm with lateral extent not to exceed 7 mm. Stage IA is further subdivided into stage IA1 with stromal invasion less than 3 mm and IA2 with invasion 35 mm in depth. Young patients with microinvasive squamous cell carcinoma of the cervix who desire future fertility can be treated with conization alone, provided that certain strict criteria are met. The cone specimen should be properly excised and then evaluated by an experienced pathologist. The tumor must meet the criteria for stage IA1 disease with invasion less than 3 mm and a lateral extent less than 7 mm. The cone margins must be negative, and there should be no lymphvascular space invasion.
Question 353:
A22-year-old nulliparous woman who desires future fertility is found to have a pap smear consistent with high-grade squamous intraepithelial lesion (HGSIL). The test you performed above was inadequate. What would be your next step in management?
A. transvaginal ultrasound (TVUS)
B. endometrial dilation and curettage
C. ECC
D. cold knife cervical conization
E. repeat pap smear in 3 months
Correct Answer: D Section: (none)
Explanation: Current American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines for treating a pap smear consistent with HGSIL is to perform colposcopy with directed biopsies if a lesion is seen. Routine pap smear in 1 year is an unacceptable option for this patient given her increased risk for developing cervical cancer. Random biopsies have a high false negative rate if there is no visible lesion to biopsy, thus, are not helpful. The pap smear is a screening test of the cervix, not the endometrium. There is no reason to suspect that this patient has endometrial pathology, therefore, an endometrial biopsy is not warranted. HPV testing is not recommended for high-grade pap smears. All high-grade pap smears require further investigation with colposcopy regardless of HPV status. If colposcopy is unsatisfactory, meaning no lesion is identified, the full transformation zone is not visualized or the full extent of the lesion is not identified, then a diagnostic excisional procedure is warranted. A loop excisional electrocautery procedure (LEEP) would be appropriate. However, note that if your suspicion for cancer is high, the cauterized edges from a LEEP procedure can complicate the pathologic assessment of positive margins. A cold knife cervical conization can be performed in the operating room as an outpatient surgery and provides the best surgical specimen for pathologic evaluation. In this case, a TVUS, endometrial dilation, and curettage, and ECC are all inappropriate options since they do not accurately evaluate the cervix, which is the primary site of concern. This patient has, by definition, microinvasive cervical cancer. Approximately 1015% of patients in the United States with stage I cervical cancer will have a microinvasive cancer. Microinvasive cancer is defined as stage IA with invasion limited to a depth of 5 mm with lateral extent not to exceed 7 mm. Stage IA is further subdivided into stage IA1 with stromal invasion less than 3 mm and IA2 with invasion 35 mm in depth. Young patients with microinvasive squamous cell carcinoma of the cervix who desire future fertility can be treated with conization alone, provided that certain strict criteria are met. The cone specimen should be properly excised and then evaluated by an experienced pathologist. The tumor must meet the criteria for stage IA1 disease with invasion less than 3 mm and a lateral extent less than 7 mm. The cone margins must be negative, and there should be no lymphvascular space invasion.
Question 354:
A22-year-old nulliparous woman who desires future fertility is found to have a pap smear consistent with high-grade squamous intraepithelial lesion (HGSIL). Initial management should be which of the following?
A. routine pap smear in 1 year
B. random cervical biopsies
C. colposcopy
D. endometrial biopsy
E. human papilloma virus (HPV) testing
Correct Answer: C Section: (none)
Explanation: Current American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines for treating a pap smear consistent with HGSIL is to perform colposcopy with directed biopsies if a lesion is seen. Routine pap smear in 1 year is an unacceptable option for this patient given her increased risk for developing cervical cancer. Random biopsies have a high false negative rate if there is no visible lesion to biopsy, thus, are not helpful. The pap smear is a screening test of the cervix, not the endometrium. There is no reason to suspect that this patient has endometrial pathology, therefore, an endometrial biopsy is not warranted. HPV testing is not recommended for high-grade pap smears. All high-grade pap smears require further investigation with colposcopy regardless of HPV status. If colposcopy is unsatisfactory, meaning no lesion is identified, the full transformation zone is not visualized or the full extent of the lesion is not identified, then a diagnostic excisional procedure is warranted. A loop excisional electrocautery procedure (LEEP) would be appropriate. However, note that if your suspicion for cancer is high, the cauterized edges from a LEEP procedure can complicate the pathologic assessment of positive margins. A cold knife cervical conization can be performed in the operating room as an outpatient surgery and provides the best surgical specimen for pathologic evaluation. In this case, a TVUS, endometrial dilation, and curettage, and ECC are all inappropriate options since they do not accurately evaluate the cervix, which is the primary site of concern. This patient has, by definition, microinvasive cervical cancer. Approximately 1015% of patients in the United States with stage I cervical cancer will have a microinvasive cancer. Microinvasive cancer is defined as stage IA with invasion limited to a depth of 5 mm with lateral extent not to exceed 7 mm. Stage IA is further subdivided into stage IA1 with stromal invasion less than 3 mm and IA2 with invasion 35 mm in depth. Young patients with microinvasive squamous cell carcinoma of the cervix who desire future fertility can be treated with conization alone, provided that certain strict criteria are met. The cone specimen should be properly excised and then evaluated by an experienced pathologist. The tumor must meet the criteria for stage IA1 disease with invasion less than 3 mm and a lateral extent less than 7 mm. The cone margins must be negative, and there should be no lymphvascular space invasion.
Question 355:
A37-year-old woman (gravida 3, para 3) presents with a 4-month history of postcoital spotting On pelvic examination, you visualize a 2-cm friable lesion on the anterior lip of the cervix. The next most appropriate step is which of the following?
A. colposcopy
B. pap smear
C. office biopsy of the cervical lesion
D. cervical cone biopsy
E. metronidazole vaginal cream followed by re-examination
Correct Answer: C Section: (none)
Explanation:
An office biopsy of the cervical lesion should be taken immediately when a gross lesion is seen on physical examination. For smaller, less distinct lesions, colposcopy may be helpful in determining the best area to biopsy, but it is not always necessary for larger, distinct, gross lesions. Apap smear can be performed, but it cannot be relied on to detect invasive cervical cancer. Cervical cone biopsy is not indicated at this time, particularly because the diagnosis can be made by less invasive means with an office biopsy. Also, if a cone biopsy is performed and the cancer is invasive or more extensive than originally thought, a cone biopsy may affect the oncologist's ability to perform a radical hysterectomy or alter the effectiveness of vaginal brachytherapy. Finally, the use of metronidazole vaginal cream is not indicated in this patient since there is no evidence of a vaginal infection.
Question 356:
In your internal medicine clinic you are caring for a 42-year-old woman with hereditary nonpolyposis colon cancer (HNPCC), Lynch syndrome II, which is a hereditary, autosomal dominant, cancer syndrome that results from a mutation in a mismatch deoxyribonucleic acid (DNA) repair gene. These patients have a lifetime risk of colon cancer nearly 6080%, but are also at risk for several other malignancies.
For which gynecologic malignancy is this woman most at risk?
A. ovarian cancer
B. breast cancer
C. cervical cancer
D. vulvar cancer
E. endometrial cancer
Correct Answer: E Section: (none)
Explanation:
Women with HNPCC, Lynch syndrome II have a 2040% lifetime risk of endometrial cancer. These women tend to get endometrial cancer at a much earlier age (median 46 years) compared to the general population (median 63 years). These women are also at risk for carcinomas of the ovary, breast, stomach, small bowel, pancreas, biliary tract, and transitional cell tumors of the urinary tract. Because of the inordinately high risk for endometrial and ovarian cancer in these patients, prophylactic hysterectomy and bilateral salpingo-oophorectomies are offered to women with this syndrome after the completion of childbearing.
Question 357:
You are consulted by a 55-year-old asymptomatic postmenopausal woman who has been on tamoxifen for 2 years following a diagnosis of breast cancer. She has no other risk factors for endometrial cancer but she was searching the Internet and found information about the risks of tamoxifen therapy. She inquires about endometrial cancer screening. You tell her that for asymptomatic woman on tamoxifen, the screening recommendations for endometrial cancer are which of the following?
A. yearly pelvic ultrasounds
B. yearly endometrial biopsies
C. yearly gynecologic examinations
D. yearly pelvic CT scans
E. yearly hysteroscopy
Correct Answer: C Section: (none)
Explanation: The current American College of Obstetricians and Gynecologists guidelines for screening women on tamoxifen for endometrial cancer state that no screening except for routine yearly gynecologic examinations should be performed in asymptomatic women. In symptomatic women with vaginal bleeding on tamoxifen therapy, endometrial biopsy is recommended. Tamoxifen directly affects the endometrium, and a pelvic ultrasound will reveal a thickened endometrium in 75% of asymptomatic women. The most common changes to the endometrium include benign cystic glandular dilation, stromal edema, endometrial hyperplasia, and polyps. Approximately 2030% of women will develop benign endometrial and endocervical polyps. Women on tamoxifen have a two-to threefold increased risk for endometrial cancer. Given the high rate of benign changes in the endometrium from tamoxifen, the usefulness of TVUS and endometrial biopsy is drastically diminished. In the setting of tamoxifen, ultrasound has only a 9% positive predictive value. However, the negative predictive value is 99%, meaning that if the ultrasound is normal, you may be 99% certain that there is no disease present. CT scans in general are less effective than ultrasound at evaluating the endometrial cavity, and they are not recommended for screening. Hysteroscopy will allow direct visualization with directed biopsy of the abnormal endometrium. However, again, the majority of lesions in women on tamoxifen will be benign, and a large number of hysteroscopies would be performed with the detection of very few cancers. Thus, this is not cost-effective and is a low yield diagnostic procedure in this group of women. Also, there is some debate as to whether hysteroscopy in the presence of endometrial cancer increases the risk for positive cytology and leads to a seeding of the peritoneal cavity with endometrial cancer cells by efflusing cancer cells from the endometrium out through the Fallopian tubes into the abdominal cavity.
Question 358:
A 61-year-old postmenopausal woman, who has been on continuous combined hormone replacement therapy for 5 years, presents to your office complaining of vaginal bleeding.
Which of the following is the most appropriate next step in her management?
A. pap smear
B. endocervical curettage (ECC)
C. pelvic ultrasound
D. endometrial biopsy
E. dilation and curettage
Correct Answer: D Section: (none)
Explanation:
Vaginal bleeding in a postmenopausal woman may be caused by numerous etiologies including an endometrial polyp, endometrial hyperplasia, atrophic endometrium, a submucosal fibroid, or endometrial cancer to name a few. In this group of women, endometrial cancer must be ruled out. Although this woman may need a pap smear as part of her routine gynecologic screening, a pap smear is inadequate to rule out the diagnosis of endometrial cancer. ECC is a sampling of the endocervical canal, not of the endometrium. Thus, again, an ECC is not adequate to rule out endometrial cancer. The ECC is more commonly used in the workup for cervical dysplasia to assess extension into the cervical canal. Athickened endometrial stripe on pelvic ultrasound can aid in making the diagnosis of an endometrial abnormality, but the ultrasound itself is not diagnostic for endometrial cancer. Athickened endometrium on ultrasound may be the result of a submucosal fibroid, hyperplasia, a polyp, or endometrial cancer. A dilation and curettage is an outpatient surgical procedure that involves dilation of the cervix and a thorough sampling of the endometrium with a curette. This procedure will obtain adequate endometrial tissue to make a diagnosis of tissue. In general, this procedure is reserved for patients in which endometrial biopsy is unsuccessful or for patients who have continued symptoms with a negative endometrial biopsy. Endometrial biopsy is a simple office procedure for sampling the endometrium, and it is 95% accurate. Thus, it is the preferred method of sampling the endometrium to rule out endometrial cancer.
Question 359:
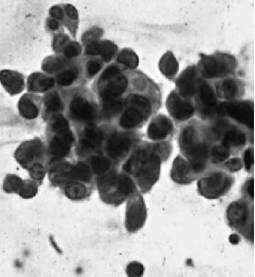
A 42-year-old woman who previously underwent a vaginal hysterectomy for persistent cervical dysplasia presents to your office for vaginal cytology. Her vaginal cytology is shown in Figure.
On speculum examination, you visualize a 1 × 1 cm lesion at the left vaginal fornix. The lesion is acetowhite, slightly raised, with coarse punctation and bizarre branching vessels. You take a biopsy of the lesion and the pathology returns consistent with vaginal intraepithelial neoplasia (VAIN) 3, suspicious for invasion.
Which of the following is your next step in management?
A. carbon dioxide (CO2) laser
B. wide local excision of the lesion
C. intravaginal 5-flourouracil (5-FU)
D. intravaginal estrogen cream
E. total vaginectomy
Correct Answer: B Section: (none)
Explanation:
VAIN is frequently found in women who have a history of cervical dysplasia. Although the etiology of VAIN has not been thoroughly elucidated, like cervical intraepithelial neoplasia (CIN), it is thought that HPV is the carcinogenic agent. Thus, when vaginal cytology is abnormal, the evaluation is very similar to that of an abnormal pap smear. It is important to assess the histologic severity and the extent of the lesion. To do this, the next step in management is a thorough colposcopic evaluation of the entire vaginal canal, especially because many patients will have multifocal disease. During colposcopy the application of acetic acid (4%) is useful. The speculum should be fully inserted to visualize the upper vagina and then slowly removed while rotating the speculum, being careful to view the entire vaginal mucosal surface. Most vaginal lesions are not grossly visible. However, a raised white epithelium may occasionally be seen. If a lesion is visible, then directed biopsy of the lesion is indicated to confirm the diagnosis. The image provided shows HGSIL. In the presence of high-grade vaginal cytology, repeat cytology in 6 months, and observation are not viable management options given the concern for carcinoma in situ or for invasive carcinoma of the vagina. Random vaginal biopsies are also not likely to be helpful since they will most likely miss the involved area and lead to a false negative result. Intravaginal estrogen cream is reserved for postmenopausal women with vaginal atrophy and low-grade VAIN without evidence of invasion. Estrogen is not a treatment for VAIN 3, or high-grade VAIN.
Question 360:
A 42-year-old woman who previously underwent a vaginal hysterectomy for persistent cervical dysplasia presents to your office for vaginal cytology. Her vaginal cytology is shown in Figure.
Which of the following is the most appropriate next step in management?
A. repeat vaginal cytology in 6 months
B. observation
C. random vaginal biopsies
D. intravaginal estrogen cream followed by repeat cytology
E. colposcopic examination of the vaginal canal
Correct Answer: E Section: (none)
Explanation: VAIN is frequently found in women who have a history of cervical dysplasia. Although the etiology of VAIN has not been thoroughly elucidated, like cervical intraepithelial neoplasia (CIN), it is thought that HPV is the carcinogenic agent. Thus, when vaginal cytology is abnormal, the evaluation is very similar to that of an abnormal pap smear. It is important to assess the histologic severity and the extent of the lesion. To do this, the next step in management is a thorough colposcopic evaluation of the entire vaginal canal, especially because many patients will have multifocal disease.
During colposcopy the application of acetic acid (4%) is useful. The speculum should be fully inserted to visualize the upper vagina and then slowly removed while rotating the speculum, being careful to view the entire vaginal mucosal surface. Most vaginal lesions are not grossly visible. However, a raised white epithelium may occasionally be seen. If a lesion is visible, then directed biopsy of the lesion is indicated to confirm the diagnosis. The image provided shows HGSIL. In the presence of high-grade vaginal cytology, repeat cytology in 6 months, and observation are not viable management options given the concern for carcinoma in situ or for invasive carcinoma of the vagina. Random vaginal biopsies are also not likely to be helpful since they will most likely miss the involved area and lead to a false negative result. Intravaginal estrogen cream is reserved for postmenopausal women with vaginal atrophy and low-grade VAIN without evidence of invasion. Estrogen is not a treatment for VAIN 3, or high-grade VAIN.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.