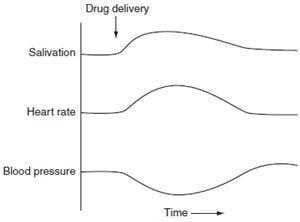
In a study of a new drug, the agent was administered to anesthetized animals while blood pressure, heart rate, and salivation were recorded. The results of a typical experiment are shown in below figure. What is the best characterization of this new agent?
A. alpha-adrenoceptor agonist
B. alpha-adrenoceptor antagonist
C. cholinesterase inhibitor
D. direct-acting muscarinic agonist
E. ganglionic nicotinic agonist
Correct Answer: D
Section: Pharmacology Salivary glands contain muscarinic receptors, primarily of the M3 subtype, that receive parasympathetic innervation. Direct-acting agonists such as bethanechol and indirect agents such as neostigmine mimic parasympathetic nerve stimulation. Blood vessel endothelial cells contain M3 receptors that are not innervated, but respond to circulating directacting muscarinic agonists. When these endothelial receptors are activated, nitric oxide synthesis is stimulated and smooth muscle relaxation occurs promptly with vasodilation and a drop in blood pressure. Because no nerve endings are present, indirect-acting cholinomimetics such as cholinesterase inhibitors do not have this vasodilating effect. In the presence of hypotension induced by a direct-acting muscarinic agonist, a strong compensatory reflex originates in the baroreceptors and results in tachycardia. In the case of cholinesterase inhibitors, the normal heart rate slowing effect of the vagus is amplified and at normal doses, bradycardia results. The effect of the new drug illustrated in figure is most consistent with a direct-acting muscarinic agonist (choice D). Alpha receptor ligands (choices A and B) have little effect on salivation, although indirectly acting agents like ephedrine can cause a sensation of dry mouth. However, ephedrine causes increased blood pressure. Aganglionic stimulant drug (choice E) causes increased salivation but also increases sympathetic discharge to the blood vessels and results in increased, not decreased, blood pressure.
Question 102:
A 75-year-old man has prostate cancer that has metastasized to bone. He is receiving hormonal therapy to slow progression of the neoplasm and codeine by mouth for pain when it is absolutely required, but still complains of severe pain. What should be given to this patient to address his symptom?
A. a strong NSAID such as naproxen as needed to supplement his codeine therapy
B. additional codeine when he complains
C. aspirin, and he should be told that additional narcotics cannot be used because he would become tolerant of their analgesic action
D. morphine in a long-acting oral preparation on a regular schedule and parenteral morphine when pain breaks through
E. parenteral morphine when pain requires it
Correct Answer: D
Section: Pharmacology Pain of malignancy is still a badly undertreated condition, due to misunderstanding of the nature of opioid tolerance and addiction and an unwillingness to deal with the complications of prescribing controlled substances. Codeine has limited maximum efficacy, so additional doses of this drug (choice B) are unlikely to control this patient's pain. It was previously thought that regular use of strong opioids for any purpose inevitably led to tolerance and a loss of analgesic effect, as well as addiction (choice C). However, excellent clinical studies have shown that this is not the case. Regular use as opposed to as-needed use) of small to moderate doses of opioids effectively controls pain in most cases without causing tolerance or addiction. In fact, restricting opioids to use only when absolutely needed results in larger total analgesia requirements and greater toxicity. Use of NSAIDs (choice A) should be started early, when pain is mild and supplemented with oral opioids, such as codeine, as soon as it becomes necessary. NSAIDs are not adequate at this stage of this patient's disease. Parenteral morphine, given when necessary (choice E), is as not as effective as regularly scheduled morphine and leads to greater drug toxicity.
Question 103:
A 38-year-old man has been treated for myasthenia gravis with pyridostigmine and propantheline for 8 years. He has had the "flu" for 10 days and his wife calls reporting that he now has serious muscle weakness. What should be administered after admitting this patient to the emergency department?
A. atropine to reverse the effects of an overdose
B. a test dose of edrophonium
C. pralidoxime on the assumption that he inadvertently overdosed
D. the daily dose of pyridostigmine on the assumption that he forgot to take his medication
E. tubocurarine
Correct Answer: B
Section: Pharmacology Myasthenia gravis is an autoimmune disease attributable to an impairment of nicotinic receptor function at the neuromuscular junction by antireceptor antibodies. Treatment consists of increasing the junctional concentration of acetylcholine with a carbamate anticholinesterase such as pyridostigmine. Infections such as influenza may change the anticholinesterase dose requirement in myasthenia either up or down. As in this patient, the problem is to distinguish whether the muscle weakness is attributable to myasthenic crisis (too little medication) or cholinergic crisis (too much medication); both conditions cause muscle weakness. The safest definitive method is to administer a small dose of the short-acting anticholinesterase edrophonium (choice B). If the patient is in myasthenic crisis, an immediate improvement in muscle function should be evident. If the patient is in cholinergic crisis, the patient's condition may worsen, but because the duration of action for edrophonium is only 510 min, this test provides less risk than other alternatives. Parenteral atropine should be available to treat excess parasympathetic activity. Atropine for symptoms of parasympathetic overdose (choice A) is inappropriate because this patient is being treated with the muscarinic antagonist propantheline and atropine will have no effect on his muscle weakness. Administration of pralidoxime (choice C) is incorrect because pralidoxime is useful for reactivation of cholinesterase only in the case of recent organophosphate intoxication. Administration of pyridostigmine (choice D) is unwise because a patient in cholinergic crisis is put at risk of exacerbation and extension of the toxic episode for a significant period of time. Administration of a test dose of a long-acting agent such as tubocurarine (choice E) to elicit muscle weakness is a provocative test that is dangerous and does not provide definitive evidence for diagnosis.
Question 104:
A 23-year-old woman is admitted to the hospital suffering from palpitations and syncopal episodes (fainting spells). She is found to be hypotensive and her ECG shows a very rapid AV nodal reentrant tachycardia. Which of the following drugs provides appropriate acute treatment for this condition?
A. adenosine
B. bethanechol
C. isoproterenol
D. metoprolol
E. procainamide
Correct Answer: A
Section: Pharmacology The current drug of choice for acute AV nodal reentrant tachycardia (a supraventricular tachycardia [SVT]) is the nucleoside adenosine. This agent, when given as a bolus, causes marked hyperpolarization of AV node tissue and transiently blocks conduction of AV node action potentials. This abolishes the reentrant impulse and allows normal sinus rhythm to be reestablished. The half-life of adenosine is about 3 seconds and the duration of action of the dose used is about 15 seconds, so toxicities from this therapy are minimal. Calcium channel blockers such as verapamil and diltiazem are also effective in SVT. Bethanechol (choice B) is a muscarinic agonist and produces hypotension and other muscarinic effects. It is ineffective in SVT. Isoproterenol (choice C) is a beta-selective adrenoreceptor agonist that causes hypotension and reflex sympathetic discharge to the heart, along with direct stimulation. It is more likely to cause than to abolish arrhythmias. Metoprolol (choice D) slows AV conduction and might abolish the AV reentrant rhythm. However, beta blockers are not very effective in converting preexisting SVT. Procainamide (choice E) and related group 1A antiarrhythmic drugs are not as effective as adenosine in converting SVT to normal sinus rhythm and much more toxic.
Question 105:
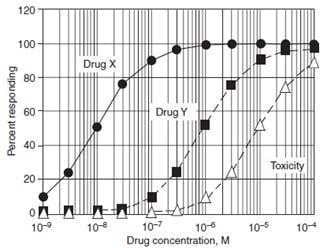
Figure shows the quantal population doseresponse curves for the therapeutic and toxic effects of drugs X and Y. Both drugs are agonists at the same receptor to produce the therapeutic response, and the maximum responses obtained with each agent are the same. The toxicity curve in the figure shows the superimposed toxic response curves for drugs X and Y; they are identical in terms of the concentration dependence. Which of the following statements is most correct?
A. At 1 × 10-5 M both drugs cause adverse effects in 90100% of patients.
B. Drug X has a larger therapeutic index than drug Y.
C. Drug X is more efficacious than drug Y.
D. Drug Y is more potent than drug X.
E. Drug Y is safer than drug X.
Correct Answer: B
Question 106:
A 78-year-old man has ankle edema, tachycardia, and shortness of breath on mild exercise. His blood pressure is 155/98. He has been diagnosed with hypertension and mild heart failure. Which of the following regimens is most appropriate for starting therapy?
A. captopril plus dobutamine
B. captopril plus hydralazine
C. enalapril plus hydrochlorothiazide
D. furosemide plus spironolactone
E. losartan plus hydralazine
Correct Answer: C
Section: Pharmacology The combination of an ACE inhibitor and a diuretic is rational for this patient with hypertension and mild heart failure as both drugs are effective for both conditions. Furthermore, ACE inhibitors have been shown to slow or stop the progression of heart failure and thiazide diuretics have been shown to be among the cheapest and most effective agents for hypertension. If this combination is not sufficiently active to control the heart failure, a loop diuretic mightbe substituted for the thiazide. Dobutamine (choice A) is a parenteral drug for acute failure. Hydralazine (choices B, E) is a vasodilator that causes tachycardia and usually requires concurrent administration of a beta blocker. Use of two diuretics choice D) is probably unnecessary in this early stage of failure and is not the most effective therapy for hypertension.
Question 107:
On the basis of their mechanisms of action, which of the following combinations of drugs produces a beneficial additive or synergistic effect in therapy when each agent is present at its maximum effective concentration?
A. chlortetracycline plus amoxicillin
B. clomiphene plus chorionic gonadotropin
C. lovastatin plus cholestyramine
D. pentazocine plus morphine
E. succinylcholine plus atracurium
Correct Answer: C
Section: Pharmacology The hydroxymethylglutaryl-CoA (HMGCoA) reductase inhibitor lovastatin and the bile acid-binding resin cholestyramine (choice C) lower the concentration of cholesterol in the blood by different mechanisms. Because they act by different mechanisms, combination therapy is at least additive. The combination of chlortetracycline and amoxicillin (choice A) results in antagonism of amoxicillin's antibacterial action. The beta-lactam cell wall synthesis inhibitors such as the penicillins and cephalosporins are bactericidal, but are effective primarily when the bacteria proliferate rapidly. Tetracyclines are bacteriostatic agents that slow or inhibit the growth of bacterial cells by inhibiting protein synthesis. The combination of clomiphene and chorionic gonadotropin (choice B) does not produce any beneficial additive action. Both agents are used to treat female infertility. Clomiphene is an estrogen-receptor partial agonist that functions at the level of the hypothalamus to stimulate release of gonadotropinreleasing hormone (GnRH). The increased release of GnRH results in increased release of the gonadotropins LH and FSH from the anterior pituitary. This results in stimulation of ovulation. Administration of chorionic gonadotropin also stimulates ovulation. Because both preparations function through increases in gonadotropin levels and both are present at their maximum effective concentrations, a beneficial additive effect is unlikely. The combination of pentazocine and morphine (choice D) does not produce a beneficial interaction. Pentazocine exerts its pain-relieving activity by a weak (partial) agonist action at mu-opioid receptors. Morphine is a full agonist at the same receptors. When the two analgesic agents are combined, pentazocine acts as an antagonist for morphine at mu- receptors. The result is precipitation of withdrawal in addicted patients, and dysphoria and loss of morphine analgesia in nonaddicted patients. Succinylcholine and atracurium (choice E) are both skeletal musclerelaxing agents that block muscle contraction by actions at the neuromuscular junction. Succinylcholine is a depolarizing blocker that acts as an agonist at the nicotinic receptor. Atracurium is a competitive antagonist at the same receptor. Because they both act at the same receptor and are present at their effective concentrations, atracurium interferes with the action of succinylcholine.
Question 108:
A 20-year-old man suffers a broken arm in a bicycle accident. After a cast is applied, he is to be discharged from the emergency department with a prescription for an analgesic to be used if over-thecounter acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs) are not effective in providing pain relief. Which of the following is the best choice for prescription pain relief in this case?
A. codeine
B. diphenoxylate
C. meperidine
D. methadone
E. morphine
Correct Answer: A
Section: Pharmacology Excellent analgesia and significant addictive properties are associated with drugs that act at mu-type opioid receptors. Of the analgesics listed, codeine is a weak agonist at mureceptors, whereas the other opioid analgesics listed (choices C, D, and E) are full agonists. Therefore codeine (choice A) is less efficacious but also has the lowest addiction and abuse liability; it is therefore the agent of choice within this list. Diphenoxylate (choice B) is a congener of meperidine (and the primary component of Lomotil) that is used to control GI motility in diarrhea. At therapeutic dose levels, neither analgesia nor addiction is observed. Meperidine (choice C) is a synthetic mu-opioid receptor agonist with high- addiction liability. Methadone (choice D) is a mu-opioid receptor agonist with good oral efficacy and a long plasma half-life (1540 h). It is used in the treatment of opioid addiction and for severe cancer pain. Morphine (choice E) is the prototype muopioid receptor agonist and possesses highaddiction liability.
Question 109:
A 57-year-old obese woman has Type II (noninsulindependent) diabetes mellitus of 15 years duration. Because her hyperglycemia is not well controlled with diet and oral hypoglycemic agents, she selfadministers insulin by injection. She comes to her physician's office with a fever and a draining external ear infection; Pseudomonas aeruginosa is cultured from the drainage fluid. Which of the following insulin regimens most closely mimics insulin release from a normally functioning pancreas?
A. prebreakfast and predinner injections of lente insulin plus an injection of regular insulin if blood glucose (measured by finger-stick) exceeds 150 mg/dL
B. premeal injections of insulin lispro plus morning and evening injections of detemir insulin
C. premeal injections of NPH insulin plus an injection of insulin lispro at bedtime
D. post-meal injection of lente insulin plus a prebreakfast injection of regular insulin
E. Post-meal injections of insulin glargine
Correct Answer: B
Section: Pharmacology Anormally functioning endocrine pancreas provides a low basal level of circulating insulin and spikes of insulin release in response to the ingestion of food and subsequent elevation of blood sugar. In a diabetic, use of morning and evening injections of a very long-acting form such as lente, glargine, or detemir insulin provides a low basal level of circulating insulin. Premeal injections of rapid-acting insulin provide the spikes of circulating insulin needed to deal with the dietary glucose load. Regular insulin or insulin lispro, glulisine, or aspart is needed for this purpose. Insulin detemir and glargine are very long-acting recombinant insulins that are used to provide basal levels. They are of no value for controlling transient hyperglycemic spikes.
Question 110:
A 57-year-old obese woman has Type II (noninsulindependent) diabetes mellitus of 15 years duration. Because her hyperglycemia is not well controlled with diet and oral hypoglycemic agents, she selfadministers insulin by injection. She comes to her physician's office with a fever and a draining external ear infection; Pseudomonas aeruginosa is cultured from the drainage fluid. Which of the following drugs or drug combinations is appropriate treatment for the P. aeruginosa infection in this diabetic patient?
A. chloramphenicol
B. nafcillin plus kanamycin
C. sulfamethoxazole plus trimethoprim
D. tetracycline
E. ticarcillin plus tobramycin
Correct Answer: E
Section: Pharmacology
P. aeruginosa is an aerobic gram-negative bacterium that is frequently the causative agent in diabetic malignant external otitis. Increased susceptibility to infection in diabetics with poor glycemic control probably arises through impairment of leukocyte function. Such serious P. aeruginosa infections are best treated parenterally with a broad-spectrum beta-lactam cell wall synthesis inhibitor such as ticarcillin in combination with an aminoglycoside such as tobramycin. Chloramphenicol (choice A) is a protein synthesis inhibitor. P. aeruginosa is resistant to chloramphenicol. Nafcillin plus kanamycin (choice B) is a combination of a penicillinase-resistant penicillin plus a limitedspectrum aminoglycoside. Nafcillin is useful in treating penicillinase-producing staphylococcal infections, but does not possess a broadenough antibacterial spectrum to eradicate P. aeruginosa. Kanamycin is ineffective against P. aeruginosa and is used orally or topically, not parenterally as needed here. Sulfamethoxazole plus trimethoprim (choice C) is a combination of a folate synthesis inhibitor and a dihydrofolate reductase inhibitor that is effective in treating urinary tract infections. P. aeruginosa is resistant to this combination. Tetracycline (choice D) is a bacteriostatic protein synthesis inhibitor. When first introduced, tetracycline was effective in treating Pseudomonas, but now all strains are resistant.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.