A 4-month-old boy presents with painful progressive joint deformity (particularly the ankles, knees, elbows, and wrists), hoarse crying, and granulomatous lesions of the epiglottis and larynx leading to feeding and breathing difficulty. Biopsy of the liver indicates an accumulation of ceramides. The observed symptoms and the results of the liver biopsy are indicative of which disease?
A. Farber lipogranulomatosis
B. fucosidosis
C. Gaucher disease
D. metachromic leukodystrophy
E. Sandhoff-Jatzkewitz disease
Correct Answer: A
Section: Biochemistry Farber lipogranulomatosis is characterized by painful and progressively deformed joints and progressive hoarseness due to involvement of the larynx. Subcutaneous nodules form near the joints and over pressure points. Granulomatous lesions form in these tissues and there is an accumulation of lipid-laden macrophages. Significant accumulation of ceramide and gangliosides is observed, particularly in the liver. If these compounds accumulate in nervous tissue there may be moderate nervous dysfunction. The illness often leads to death within the first few years of life, although milder forms of the disease have been identified. Fucosidosis (choice B) is characterized by the accumulation and excretion of glycoproteins, glycolipids, and oligosaccharides- containing fucoside moieties. Symptoms of fucosidosis include psychomotor retardation, dystosis multiplex (a term referring to multiple skeletal abnormalities), growth retardation, and coarse facial features. Gaucher disease (choice C) is characterized by an accumulation of glucosylceramide (glucocerebroside). Several forms of the disease have been identified and vary in severity. Typical symptoms include hepatosplenomegaly, bone lesions, and CNS involvement. Occasionally, the lungs and other organs may be involved. Metachromic leukodystrophy (choice D) is a disorder of myelin metabolism. It is characterized by the accumulation of galactosyl sulfatide (cerebroside sulfate). Symptoms may appear at any age and include mental regression, urinary incontinence, blindness, loss of speech, peripheral neuropathy, and seizures. Sandhoff- Jatzkewitz disease (choice E) is a disorder related to Tay-Sachs disease. It is characterized by a defect in the degradation of GM2 gangliosides with symptoms of severe mental retardation, blindness, and early mortality.
Question 592:
A 25-year-old man has experienced chronic blistering and scarring of his skin when exposed to sunlight. This man is a smoker and drinks heavily, both of which exacerbate his responses to sunlight. Analysis of his urine and plasma indicates a high accumulation of complex porphyrins, predominantly uroporphyrin. The symptoms and clinical signs displayed by this patient indicate he is suffering from which of the following disorders?
A. acute intermittent porphyria (AIP)
B. hereditary coproporphyria (HCP)
C. porphyria cutanea tarda (PCT)
D. variegate porphyria
E. X-linked sideroblastic anemia
Correct Answer: C
Question 593:
An investigational diabetes treatment involving a hypoglycemia-inducing drug has been developed. This drug is designed to inhibit dipeptidylpeptidase IV (DPP IV) activity and has been shown to decrease plasma glucose concentration and pancreatic glucagon secretion. DPP IV hydrolyzes which of the following hormones such that its inhibition results in the observed effects?
A. glucagon
B. glucagon-like peptide-1 (GLP-1)
C. insulin
D. insulin-like growth factor-I (IGF-I)
E. pancreatic polypeptide
Correct Answer: B
Section: Biochemistry GLP-1 is derived from the product of the proglucagon gene. This gene encodes a preproprotein that is differentially cleaved depending on the tissue in which it is synthesized. In the gut, prohormone convertase 1/3 action leads to release of several peptides including GLP-1. On nutrient ingestion GLP- 1 is secreted from intestinal enteroendocrine Lcells. Bioactive GLP-1 consists of two forms: GLP-1(737) and GLP-1(7-36) amide, where the latter form constitutes the majority (80%) of the circulating hormone. The primary physiologic responses to GLP-1 are glucose-dependent insulin secretion, inhibition of glucagon secretion, and inhibition of gastric acid secretion and gastric emptying. The latter effect will lead to increased satiety with reduced food intake along with a reduced desire to ingest food. The action of GLP-1 at the level of insulin and glucagon secretion results in significant reduction in circulating levels of glucose following nutrient intake. The glucose-lowering activity of GLP-1 is highly transient as the halflife of this hormone in the circulation is less than 2 minutes. Removal of bioactive GLP-1 is a consequence of N-terminal proteolysis catalyzed by DPP IV. DPP IV is also known as the lymphocyte surface antigen CD26 and has numerous activities unrelated to hormone inactivation. Although targeting compounds that can inhibit the enzymatic action of DPP IV would seem like ideal candidates for treating the hyperglycemia of uncontrolled diabetes, there are several unknowns associated with DPP IV inhibition. One of these issues is the fact that GLP-1 is only one of the many known substrates for DPP IV cleavage. Thus, prolonged inhibition of DPP IV enzymatic activity may have unexpected consequences unrelated to control of hyperglycemia. DPP IV is not known to hydrolyze glucagons (choice A), insulin (choice C), IGF-I (choice D), nor pancreatic polypeptide (choice E).
Question 594:
An adult man suffered from stable angina pectoris for 15 years, during which time there was progressive heart failure and repeated pulmonary thromboembolism. On his death at age 63, autopsy disclosed enormous cardiomyopathy (1100 g), cardiac storage of globotriaosylceramide (11 mg lipid/g wet weight), and restricted cardiocytes. Which of the following lipid storage diseases would result in these clinical findings?
A. Fabry disease
B. Gaucher disease
C. Krabbe disease
D. Niemann-Pick disease (NPD) type I A
E. Tay-Sachs disease
Correct Answer: A
Question 595:
A 7-year-old boy is examined by his pediatrician because of complaints of severe cramping pain in his legs whenever he rides his bike. He also expriences nausea and vomiting during these attacks. The child has noted that the severity of the cramps is most intense after dinners that include baked potatoes or pasta, and sometimes bread. Clinical studies undertaken following a treadmill test demonstrate myoglobinuria, hyperuricemia, and increased serum bilirubin. Which of the following enzyme deficiencies is associated with these clinical findings?
A. glucose-6-phosphatase
B. glycogen synthase
C. liver glycogen debranching enzyme
D. muscle phosphofructokinase
E. muscle phosphorylase
Correct Answer: D
Section: Biochemistry A deficiency in muscle phosphofructokinase results in glycogen storage disease type VII (Tarui disease). Clinically, the symptoms seen in Tarui disease are very similar to those seen in muscle phosphorylase deficiency (choice E), glycogen storage disease type V (McArdle disease) such as exercise-induced cramping and early fatigue. There are five clinical characteristics allowing distinction between Tarui and McArdle diseases: exercise intolerance is evident in childhood, is more severe, and is associated with nausea and vomiting; the intolerance is particularly acute following meals rich in carbohydrates; hyperuricemia is more severe; compensated hemolytic anemia is evidenced by increased serum bilirubin and reticulocyte count, and lastly; an abnormal polysaccharide is present in muscle fibers. Deficiency in glucose-6-phosphatase (choice A) is one cause of glycogen storage disease type I (specifically type Ia, von Gierke disease). Classic symptoms of this deficiency include neonatal hypoglycemia and lactic acidosis. If symptoms do not appear until the third or fourth month they include hepatomegaly and hypoglycemic seizures. Liver glycogen synthase deficiency (choice B) presents with morning fatigue and ketotic hypoglycemia on fasting--both of which rapidly disappear on feeding. Symptoms can be rapidly relieved and chemical signs corrected by introducing frequent protein-rich meals and nighttime feedings of suspensions of uncooked corn starch. Deficiency in glycogen debranching enzyme (choice C) results in glycogen storage disease type III (Cori or Forbes disease). Symptoms of type III disease are short stature, variable skeletal myopathy, cardiomyopathy, hepatomegaly, and hypoglycemia.
Question 596:
A deficiency of argininosuccinate synthetase (ASD) can be suspected in a 2448-hour-old neonate with elevated serum ammonia. To discriminate the fact that the hyperammonemia is indeed due to ASD and not due to a deficiency in other urea cycle enzymes, one can assay for the serum concentration of citrulline and urinary orotic acid concentration. Which of the following would best describe the expected findings?
A. Both citrulline and orotate levels will be low.
B. Citrulline levels will be absent but orotate will be elevated.
C. Citrulline levels will be between 100300 M and orotate levels will be elevated.
D. Citrulline levels will be >1000 M, orotate will be near normal.
Correct Answer: D
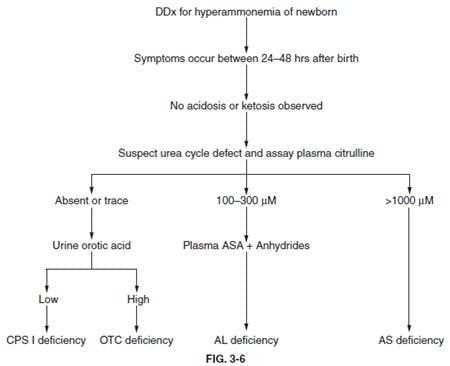
Section: Biochemistry A urea cycle disorder (UCD) is likely in a neonate that has elevated serum ammonia appearing, not before, but between 24 and 48 hours after a normal term delivery. There are three hallmark symptoms associated with UCDs. These are hyperammonemia, encephalopathy, and respiratory alkalosis. Thus, elevated serum ammonia is not, in and of itself, indicative of a specific defect in the urea cycle. An analysis of the levels of various amino and organic acids in the plasma and urine is the primary key to determining which defect led to the elevation in serum ammonia. Differential diagnosis of neonatal hyperammonemia, as a consequence of a UCD can be accomplished by measurement of plasma citrulline and urinary orotic acid levels. Shown in below figure is the standard differential diagnosis chart for determining which of four possible neonatal UCDs is the cause of the hyperammonemia.
First, the hyperammonemia appears in the absence of any significant acidosis or ketosis. If analysis of serum citrulline demonstrates that it is >1000 M it is confirmation that the clinical symptoms are due to a deficiency in ASD. In this circumstance it is not necessary to assay for levels of urinary orotic acid but they would be expected to be normal. Since citrulline levels are dramatically elevated in cases of ASD, choices A, B, and C are not correct.
Question 597:
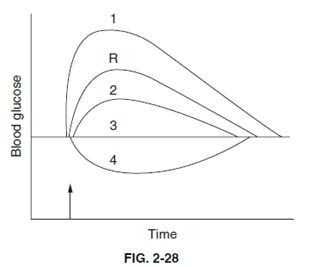
Below figure shows blood glucose levels after ingestion, at the arrow of 100 grams of glucose in a patient newly diagnosed with Type II diabetes. The curve labeled R is the patient's reference response. After curve R was obtained, the patient commenced a daily exercise regime. After several weeks of exercise a second curve was obtained. Which of the following best describes the response to glucose after exercise training?
A. curve 1
B. curve 2
C. curve 3
D. curve 4
Correct Answer: B
Section: Physiology Exercise recruits both non-insulin-dependent and insulin-dependent glucose transport proteins to the plasma membrane of active skeletal muscle cells. This effectively increases sensitivity to insulin and the response to ingested glucose is blunted after exercise training. This excludes choice E, which states that no effect can be expected from exercise and choice A (curve 1), which represents a state of lower insulin receptor sensitivity compared to the sedentary state R. Ingestion of glucose will cause an initial rise of blood glucose in both active and sedentary people (excludes choices C and D).
Question 598:
A 23-year-old female has serum electrolytes tested as part of a routine physical. The laboratory results reveal a mild degree of hypokalemia. Which of the following will promote movement of extracellular potassium into the intracellular fluid compartment and cause hypokalemia?
A. extracellular fluid hyperosmolality
B. intravenous administration of a betaadrenergic blocker
C. intravenous administration of insulin
D. metabolic acidosis
E. physical exercise
Correct Answer: C
Question 599:
Exhibit:
Please refer to the exhibit.
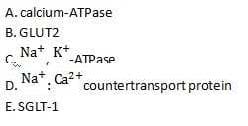
Which of the following proteins uses the sodium electrochemical gradient to actively transport a solute into
the cell?
A. A
B. B
C. C
D. D
E. E
Correct Answer: E
Section: Physiology SGLT-1 is a sodium-dependent cotransport protein that uses the sodium electrochemical gradient to actively move glucose into the cell. GLUT2 (choice B) does transport glucose, but it is a facilitated diffusion carrier that moves glucose down its concentration gradient. The Na, K-ATPase (choice C) is a primary active transport protein. It uses the energy liberated from ATP hydrolysis to actively transport sodium and potassium. It establishes and maintains the sodium electrochemical gradient. The sodium: calcium countertransport protein (choice D, also termed NCX) uses the sodium electrochemical gradient to move calcium ions out of, not into, the cell. The calcium ATPase (choice A, also termed PMCA) is a primary active transport protein that actively transports calcium out of the cell. Both NCX and PMCA serve to maintain a low intracellular calcium concentration.
Question 600:
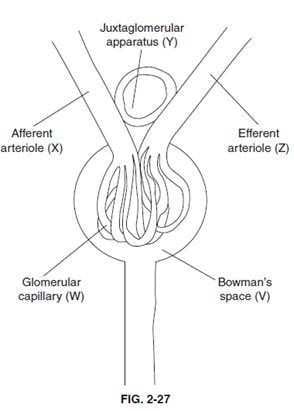
With respect to below figure, which of the following will decrease the GFR?
A. decreased hydrostatic pressure in V
B. decreased plasma protein concentration in W
C. dilation of X
D. dilation of Z
E. increased aldosterone secretion by Y
Correct Answer: D
Section: Physiology These choices revolve around the Starling forces that directly regulate glomerular filtration. Choice D is correct and choice C is incorrect because glomerular capillary pressure is regulated by the ratio of upstream (afferent arteriole) and downstream (efferent arteriole) resistance to flow. Dilation of the afferent arteriole (choice C) will increase glomerular capillary pressure and increase filtration, whereas dilation of the efferent arteriole (choice D) will decrease the pressure and thus decrease filtration. Choice A is incorrect because Bowman's space pressure normally acts to oppose filtration, hence a decreased pressure will increase filtration. Choice B is incorrect because the osmotic pressure of the plasma proteins opposes filtration, so a decreased plasma protein concentration will predictably increase filtration. Choice E is incorrect, first of all because the juxtaglomerular apparatus does not secrete aldosterone, but instead secretes renin, which ultimately can trigger aldosterone secretion from the adrenal cortex via angiotensin
II. Secondly, aldosterone is likely to trigger salt and water retention by an action on the distal nephron of the kidney, which is likely to alter the Starling forces in favor of increased glomerular filtration.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.