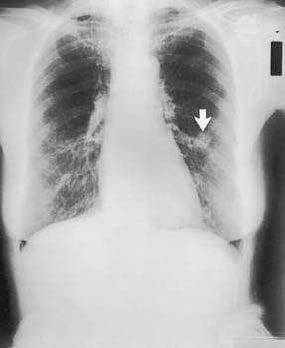
A 65-year-old woman presents to the physician's office for her yearly physical examination. She has no complaints except for a recent 10-lb weight loss. Past history is pertinent for a 40 pack-year smoking history, hypertension, asthma, and hypothyroidism. Examination reveals a thin woman with normal vital signs and unremarkable heart and abdominal examinations. Lung examination reveals mild wheezing and a few bibasilar rales. A chest x-ray is obtained and is shown in Figure. Achest x-ray obtained 3 years ago was normal. Yearly laboratory tests including a CBC, electrolytes, and lipid panels are normal.
Which of the following is the most likely diagnosis?
A. small cell lung cancer
B. tuberculosis
C. nonsmall cell lung cancer
D. hamartoma
E. abscess
Correct Answer: C
The finding of a new, irregular lesion in a patient with a long smoking history must be considered a lung carcinoma and should be managed accordingly. Nonsmall cell carcinoma is the most common lung neoplasm. Small cell carcinomas usually grow rapidly and disseminate widely by the time of diagnosis. Tuberculosis would present with systemic symptoms and apical disease on chest x-ray. Likewise, a lung abscess would be accompanied by systemic symptoms and may show air-fluid levels in the abscess cavity. A hamartoma presents as an extremely slowly growing nodule that may contain popcorn calcifications. The most appropriate test following suspicious findings on a chest x-ray would be a CT scan to evaluate further the nodule, evaluate the lymph node status, and triage subsequent diagnostic tests. If enlarged mediastinal nodes are seen, then mediastinoscopy may be indicated. Bronchoscopy may be helpful to assess for endobronchial lesions and to obtain tissue for diagnosis. Pulmonary function tests are necessary once a decision is made to consider operation. Percutaneous needle biopsy may be required to obtain tissue once CT scanning is performed.
Question 122:
A75-year-old woman is admitted to the hospital from a nursing home for abdominal pain and pneumonia.
She was noted to be short of breath with increasing cough for 2 days before admission. Treatment,
consisting of supplemental oxygen, IV antibiotics, and pulmonary toilet, is instituted, with improvement
within 2 days. On the third hospital day, her abdominal pain worsens. Examination reveals a mildly
distended abdomen with bowel sounds but no signs of peritonitis. Remainder of examination reveals a
tender bulge in the medial left thigh below the inguinal ligament. Gentle pressure causes more pain but
does not change the size or shape of the bulge. Abdominal films show a nonspecific bowel gas pattern.
Laboratory analysis shows a WBC of 13,000, decreased from 18,000 at the time of admission.
Which ofthe following is the most likely diagnosis?
A. incarcerated direct inguinal hernia
B. lymph node with abscess
C. femoral artery aneurysm
D. incarcerated indirect inguinal hernia
E. incarcerated femoral hernia
Correct Answer: E
The diagnosis of an incarcerated hernia must be considered in the differential diagnosis of a patient with abdominal symptoms and a nonreducible inguinal bulge. Femoral hernia presents as a bulge below the inguinal ligament medial to the femoral artery. Direct or indirect inguinal hernias would present above the inguinal ligament. An aneurysm of the femoral artery should be pulsatile. If there is concern for an aneurysm, a Doppler ultrasound examination may be diagnostic. Alymph node with abscess may present as a tender, nonreducible mass, but should be accompanied by additional adenopathy and a source of the infection.
Question 123:
A 45-year-old man presents to the physician's office for evaluation of a skin lesion on his abdomen. He states that the lesion has been present for 1 year, but has recently enlarged over the last 2 months. The mass is nontender, and he is otherwise asymptomatic. Past history is unremarkable. Examination reveals a 3-cm, pigmented, irregular skin lesion located in the left lower quadrant of the abdomen, as shown in Figure. Heart, lung, and abdominal examination are normal. There are no palpable cervical, axillary, or inguinal lymph nodes. Chest x-ray and liver function tests are normal.
Which of the following is the most appropriate next step in management?
A. wide excision with 2 cm margin
B. wide excision with 2 cm margin and SLN mapping
C. shave biopsy
D. excisional biopsy with 12 mm margins
E. Mohs' surgical excision
Correct Answer: D
Amulticolored brown or black pigmented lesion with irregular borders should raise the concern of melanoma. Squamous cell carcinoma usually presents as an erythematous papular nodule. The most common type of basal carcinoma presents as an ulcerative, well-circumscribed nodule, although occasionally it may be pigmented and confused with melanoma. Merkel cell carcinoma appears as red to purple papular nodules. Keratoacanthoma is a well-circumscribed keratotic lesion that may regress without treatment. The most appropriate next step is to perform an excisional biopsy with narrow margins to confirm the diagnosis and determine depth of invasion. Shave biopsy would yield a pathologic diagnosis, but would not allow appropriate staging and is never recommended. The margin of resection and determination of lymph node management would depend on the depth of invasion of the melanoma measured in millimeters. Therefore, wide excision is not recommended until the depth of invasion of the lesion is determined by excisional biopsy with narrow margins. Mohs' surgery should be considered for nonmelanoma tumors but is not recommended for melanoma.
Question 124:
A 45-year-old man presents to the physician's office for evaluation of a skin lesion on his abdomen. He states that the lesion has been present for 1 year, but has recently enlarged over the last 2 months. The mass is nontender, and he is otherwise asymptomatic. Past history is unremarkable. Examination reveals a 3-cm, pigmented, irregular skin lesion located in the left lower quadrant of the abdomen, as shown in Figure. Heart, lung, and abdominal examination are normal. There are no palpable cervical, axillary, or inguinal lymph nodes. Chest x-ray and liver function tests are normal.
Which of the following is the most likely diagnosis?
A. squamous cell carcinoma
B. basal cell carcinoma
C. Merkel cell carcinoma
D. melanoma
E. keratoacanthoma
Correct Answer: D
Amulticolored brown or black pigmented lesion with irregular borders should raise the concern of melanoma. Squamous cell carcinoma usually presents as an erythematous papular nodule. The most common type of basal carcinoma presents as an ulcerative, well-circumscribed nodule, although occasionally it may be pigmented and confused with melanoma. Merkel cell carcinoma appears as red to purple papular nodules. Keratoacanthoma is a well-circumscribed keratotic lesion that may regress without treatment. The most appropriate next step is to perform an excisional biopsy with narrow margins to confirm the diagnosis and determine depth of invasion. Shave biopsy would yield a pathologic diagnosis, but would not allow appropriate staging and is never recommended. The margin of resection and determination of lymph node management would depend on the depth of invasion of the melanoma measured in millimeters. Therefore, wide excision is not recommended until the depth of invasion of the lesion is determined by excisional biopsy with narrow margins. Mohs' surgery should be considered for nonmelanoma tumors but is not recommended for melanoma.
Question 125:
A 62-year-old woman presents to the physician's office with complaints of constipation. She has had constipation for the last 6 months, which has worsened over the last month, associated with mild bloating. She noted that her stool has become "pencil thin" in the last month, with occasional blood, but she continues to have bowel movements daily. Past history is unremarkable. Examination reveals normal vital signs and heart and lung examination. Abdominal examination reveals mild fullness, especially in the lower quadrants. Rectal examination shows no rectal masses, but the stool is hematest positive. Abarium xray is obtained, and one view is shown in Figure.
Which of the following is the most appropriate next step in management?
A. proctoscopy and passage of a rectal tube
B. proctoscopy and biopsy
C. colonoscopy
D. endoscopic dilation of the stricture
E. NPO, IV fluids, and antibiotics
Correct Answer: B
The history of decreasing caliber of the stool with evidence of bleeding is highly suggestive of rectal carcinoma. The barium x-ray shows a near-obstructing lesion of the rectum with an "apple core" appearance of cancer. Diverticulitis does not occur in the rectum due to the lack of diverticular disease at this site. Ischemia usually does not involve the rectum due to its more abundant blood supply than the colon. The barium enema findings of sigmoid volvulus would show a smooth, tapering, so-called "bird's beak" at the rectosigmoid junction, rather than an irregular lesion in the midrectum as shown in the figure. Crohn's disease would be expected to show fistulas, either by examination or radiography. The next step in management is to confirm the diagnosis by proctoscopy and biopsy. Colonoscopy may not be feasible given the degree of the stricture, and endoscopic dilation is not routine and would not be recommended. Experience with placement of stents is accruing, but endoscopic placement of stents is not yet widely available. Because this process does not represent a volvulus, placement of a rectal tube is not required. Administration of antibiotics would be considered in the perioperative period, but not before making a histologic diagnosis.
Question 126:
A 62-year-old woman presents to the physician's office with complaints of constipation. She has had constipation for the last 6 months, which has worsened over the last month, associated with mild bloating. She noted that her stool has become "pencil thin" in the last month, with occasional blood, but she continues to have bowel movements daily. Past history is unremarkable. Examination reveals normal vital signs and heart and lung examination. Abdominal examination reveals mild fullness, especially in the lower quadrants. Rectal examination shows no rectal masses, but the stool is hematest positive. Abarium xray is obtained, and one view is shown in Figure.
Which of the following is the most likely diagnosis?
A. Crohn's disease
B. ischemia with stricture
C. rectal carcinoma
D. sigmoid volvulus
E. diverticulitis with colovesical fistula
Correct Answer: C
The history of decreasing caliber of the stool with evidence of bleeding is highly suggestive of rectal carcinoma. The barium x-ray shows a near-obstructing lesion of the rectum with an "apple core" appearance of cancer. Diverticulitis does not occur in the rectum due to the lack of diverticular disease at this site. Ischemia usually does not involve the rectum due to its more abundant blood supply than the colon. The barium enema findings of sigmoid volvulus would show a smooth, tapering, so-called "bird's beak" at the rectosigmoid junction, rather than an irregular lesion in the midrectum as shown in the figure. Crohn's disease would be expected to show fistulas, either by examination or radiography. The next step in management is to confirm the diagnosis by proctoscopy and biopsy. Colonoscopy may not be feasible given the degree of the stricture, and endoscopic dilation is not routine and would not be recommended. Experience with placement of stents is accruing, but endoscopic placement of stents is not yet widely available. Because this process does not represent a volvulus, placement of a rectal tube is not required. Administration of antibiotics would be considered in the perioperative period, but not before making a histologic diagnosis.
Question 127:
A54-year-old woman presents to her physician for an opinion regarding additional therapy following curative resection of recently diagnosed colon cancer. She underwent uncomplicated sigmoid resection for invasive colon cancer 4 weeks ago. The pathology revealed carcinoma invading into, but not through, the muscularis propria, with one of eight positive mesenteric nodes. There was no evidence of liver metastases at the time of operation. Preoperative chest x-ray and CT scan of the abdomen showed no evidence of distant disease. Preoperative carcinoembryonic antigen (CEA) level was normal. Past history is positive for diabetes and mild hypertension. Examination is unremarkable except for a healing abdominal incision. Which of the following is the most appropriate recommendation regarding adjuvant therapy?
A. no therapy indicated
B. 5-fluorouracil chemotherapy
C. 5-fluorouracil chemotherapy with leucovorin
D. doxorubicin (Adriamycin) chemotherapy
E. Adriamycin chemotherapy with methotrexate and cytoxan
Correct Answer: C
The stage of colon cancer is based on the depth of invasion, nodal involvement, and distant metastases. Stage 0 represents carcinoma in situ, stage I invasion of the submucosa or muscularis propria without node involvement, stage II invasion through the muscularis propria or directly invading other organs without nodal involvement, stage III any depth of invasion with nodal metastasis, and stage IV any depth of invasion or nodal status with distant metastases. Adjuvant therapy has been shown to be beneficial in patients with stage III disease in randomized studies. The recommended regimen is 5-fluorouracil-based chemotherapy with leucovorin, rather than 5-fluorouracil alone. Adriamycin therapy, either alone or with other agents, has not been shown to be beneficial in patients with colon cancer. No adjuvant therapy would be indicated for patients with stage 0, I, or II disease, although some patients with stage II disease manifesting poor prognostic indicators may be candidates for adjuvant therapy.
Question 128:
A54-year-old woman presents to her physician for an opinion regarding additional therapy following curative resection of recently diagnosed colon cancer. She underwent uncomplicated sigmoid resection for invasive colon cancer 4 weeks ago. The pathology revealed carcinoma invading into, but not through, the muscularis propria, with one of eight positive mesenteric nodes. There was no evidence of liver metastases at the time of operation. Preoperative chest x-ray and CT scan of the abdomen showed no evidence of distant disease. Preoperative carcinoembryonic antigen (CEA) level was normal. Past history is positive for diabetes and mild hypertension. Examination is unremarkable except for a healing abdominal incision. Which of the following is the correct stage of this patient's colon cancer?
A. stage 0
B. stage I
C. stage II
D. stage III
E. stage IV
Correct Answer: D
The stage of colon cancer is based on the depth of invasion, nodal involvement, and distant metastases. Stage 0 represents carcinoma in situ, stage I invasion of the submucosa or muscularis propria without node involvement, stage II invasion through the muscularis propria or directly invading other organs without nodal involvement, stage III any depth of invasion with nodal metastasis, and stage IV any depth of invasion or nodal status with distant metastases. Adjuvant therapy has been shown to be beneficial in patients with stage III disease in randomized studies. The recommended regimen is 5-fluorouracil-based chemotherapy with leucovorin, rather than 5-fluorouracil alone. Adriamycin therapy, either alone or with other agents, has not been shown to be beneficial in patients with colon cancer. No adjuvant therapy would be indicated for patients with stage 0, I, or II disease, although some patients with stage II disease manifesting poor prognostic indicators may be candidates for adjuvant therapy.
Question 129:
A 65-year-old man presents to the physician's office for his yearly physical examination. His only complaint relates to early fatigue while playing golf. Past history is pertinent for mild hypertension. Examination is unremarkable except for trace hematest-positive stool. Blood tests are normal except for a hematocrit of
32. A UGI series is performed and is normal. A barium enema is performed, and one view is shown in the figure below.
Which of the following is the most appropriate therapy following colonoscopy?
A. proximal colostomy with mucous fistula
B. radiation therapy
C. chemotherapy
D. surgical resection and primary anastomosis
E. surgical bypass (colocolostomy)
Correct Answer: D
The clinical features of colon cancer are variable depending on the location. On the right, fatigue, as a manifestation of anemia, may be the predominant symptom; whereas, obstructive complaints may predominate for lesions on the left. In the figure, an annular or "apple core" lesion is noted, consistent with carcinoma. Radiography of diverticular disease would show numerous protrusions from the lumen, usually localized to the sigmoid colon. Lymphoma may occur in the colon, but this site of disease is rare, and widespread disease can be documented in most cases. Ischemia usually occurs at the splenic flexure, and the resultant stricture would produce a longer segment of narrowing than that usually seen with carcinoma. Patients with Crohn's disease would manifest symptoms of abdominal pain and diarrhea, and barium x-rays would show thickened bowel wall, mucosal ulcerations, and cobblestone appearance. The treatment of colon cancer in this patient would be surgical resection and anastomosis. Colostomy may be appropriate in selected patients with obstruction in an unstable patient in whom resection is not feasible. Surgical bypass would be appropriate only or palliative therapy of unresectable disease. Radiation therapy or chemotherapy without surgical resection and staging is not recommended.
Question 130:
A 75-year-old woman is brought to the emergency department from a nursing home for abdominal pain, distention, and obstipation over the last 2 days. Past history is pertinent for stroke, diabetes, atrial fibrillation, and chronic constipation. Examination reveals a temperature of 98.6°F, pulse rate 90/min and irregularly irregular, and BP 160/90 mmHg. Heart examination reveals irregularly irregular rhythm with no murmurs; lung examination reveals few bibasilar rales; and abdominal examination reveals a distended, tympanic abdomen with mild tenderness and no rebound tenderness. Plain abdominal x-rays reveal dilated loops of bowel, and a barium enema is obtained and shown in the figure below.
Which of the following is the most appropriate next step in management following NG tube decompression and resuscitation?
A. urgent sigmoid resection
B. nonoperative reduction by proctoscopy and rectal tube
C. proximal colostomy
D. urgent operative detorsion
E. nonoperative reduction by passage of well-lubricated rectal tube
Correct Answer: B
The diagnosis of sigmoid volvulus is based on the history, examination, and radiographs. Acute onset of abdominal pain, distention, and obstipation is suggestive of volvulus. Barium enema is diagnostic of sigmoid volvulus showing the characteristic tapering to a "bird's beak" pointing to the site of obstruction. Cecal volvulus would show complete filling of the left colon. Stricture as a result of ischemic colitis would show a long, narrowed segment of colon. Diverticulitis would be suggested by a different clinical presentation including fever, sepsis, and pain localized to the left lower quadrant. Obstruction from colon cancer would show an irregular narrowing of the colon segment rather than a smooth tapering. In patients who have no signs of bowel wall ischemia (e.g., rebound tenderness, sepsis, and so forth), nonoperative reduction should be attempted and would be expected to be successful in 7080% of patients. The most widely used method of reduction is proctoscopy and rectal tube placement under direct vision. Blind passage of a rectal tube may lead to perforation and is contraindicated. Operation is indicated if nonoperative reduction is unsuccessful, with operative reduction preferred, followed by delayed resection and primary anastomosis rather than sigmoid resection. Operative reduction by detorsion alone is unacceptable because of the high recurrence rate and is, therefore, combined with sigmoidopexy or sigmoidostomy. Proximal colostomy alone is contraindicated, because strangulation of the sigmoid or recurrent volvulus is not prevented.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.