A 75-year-old woman is brought to the emergency department from a nursing home for abdominal pain, distention, and obstipation over the last 2 days. Past history is pertinent for stroke, diabetes, atrial fibrillation, and chronic constipation. Examination reveals a temperature of 98.6癋, pulse rate 90/min and irregularly irregular, and BP 160/90 mmHg. Heart examination reveals irregularly irregular rhythm with no murmurs; lung examination reveals few bibasilar rales; and abdominal examination reveals a distended, tympanic abdomen with mild tenderness and no rebound tenderness. Plain abdominal x-rays reveal dilated loops of bowel, and a barium enema is obtained and shown in the figure below.
Which of the following is the most likely diagnosis?
A. ischemic colitis with stricture
B. diverticulitis with obstruction
C. cecal volvulus
D. sigmoid volvulus
E. colon cancer with obstruction
Correct Answer: D
The diagnosis of sigmoid volvulus is based on the history, examination, and radiographs. Acute onset of abdominal pain, distention, and obstipation is suggestive of volvulus. Barium enema is diagnostic of sigmoid volvulus showing the characteristic tapering to a "bird's beak" pointing to the site of obstruction. Cecal volvulus would show complete filling of the left colon. Stricture as a result of ischemic colitis would show a long, narrowed segment of colon. Diverticulitis would be suggested by a different clinical presentation including fever, sepsis, and pain localized to the left lower quadrant. Obstruction from colon cancer would show an irregular narrowing of the colon segment rather than a smooth tapering. In patients who have no signs of bowel wall ischemia (e.g., rebound tenderness, sepsis, and so forth), nonoperative reduction should be attempted and would be expected to be successful in 7080% of patients. The most widely used method of reduction is proctoscopy and rectal tube placement under direct vision. Blind passage of a rectal tube may lead to perforation and is contraindicated. Operation is indicated if nonoperative reduction is unsuccessful, with operative reduction preferred, followed by delayed resection and primary anastomosis rather than sigmoid resection. Operative reduction by detorsion alone is unacceptable because of the high recurrence rate and is, therefore, combined with sigmoidopexy or sigmoidostomy. Proximal colostomy alone is contraindicated, because strangulation of the sigmoid or recurrent volvulus is not prevented.
Question 132:
A 55-year-old man presents to the emergency department with left lower quadrant abdominal pain. The pain has been present for 1 week, but has increased in intensity over the last 2 days associated with nausea, constipation, and dysuria. Past history is unremarkable. Examination reveals a temperature of 101°F, pulse rate of 95/min, BP of 130/70 mmHg, and normal heart and lung examinations. Abdominal examination reveals fullness and marked tenderness in the left lower quadrant, with voluntary guarding and decreased bowel sounds. Laboratory tests reveal a WBC count of 18,000 with a left shift and 20 50 WBCs in the urinalysis. A CT scan of the abdomen reveals a thickened sigmoid colon with pericolonic inflammation. He is admitted to the hospital for treatment. Which of the following is the most appropriate management of this patient?
A. NPO, IV fluids, and IV antibiotics for gram-negative and anaerobic coverage
B. NPO, IV fluid hydration, followed by immediate sigmoid colon resection
C. NPO, IV fluids, and anticoagulation
D. NPO, IV fluids, evaluation of stool for Clostridium difficile toxin, and eithermetronidazole or vancomycin antibiotic therapy
E. NPO, IV fluids, initiation of bowel preparation for elective sigmoid colon resection during the current hospitalization
Correct Answer: A
The gradual onset of left lower quadrant pain over a number of days with left lower quadrant abdominal tenderness and CT scan showing sigmoid colon inflammatory changes is most consistent with diverticulitis. Acontained perforation, either due to the diverticulitis or colon cancer, should be noted on the CT scan. There is no history of antecedent antibiotic therapy to suggest the diagnosis of pseudomembranous colitis. Though WBCs were present in the urinalysis, a diagnosis of pyelonephritis cannot be made on this basis alone, because pericolonic inflammation may be responsible for the WBCs. CT scanning is very accurate in diagnosing diverticulitis, so there is no need for any additional test. Barium enema and colonoscopy should not be performed in patients with suspected acute diverticulitis. The increased intraluminal pressure from either of these examinations may lead to free rupture of a contained abscess or phlegmon, leading to emergency surgery. However, either examination, or both, should be performed after complete resolution of diverticulitis (e.g., in 6 weeks' time) to evaluate for extent of disease, complications, and carcinoma. IVP and angiography are not indicated for diverticulitis. The appropriate management in this patient with his first episode of diverticulitis is medical management with IV antibiotics for gram- negative and anaerobic bacteria. Colon resection, either immediate or elective, should not be undertaken unless the patient's condition deteriorates or recurs. Bowel preparation cannot be performed safely in patients with acute diverticulitis. Anticoagulation has no role in therapy. Metronidazole or vancomycin therapy would be appropriate for pseudomembranous colitis, but not for diverticulitis
Question 133:
A 55-year-old man presents to the emergency department with left lower quadrant abdominal pain. The pain has been present for 1 week, but has increased in intensity over the last 2 days associated with nausea, constipation, and dysuria. Past history is unremarkable. Examination reveals a temperature of 101°F, pulse rate of 95/min, BP of 130/70 mmHg, and normal heart and lung examinations. Abdominal examination reveals fullness and marked tenderness in the left lower quadrant, with voluntary guarding and decreased bowel sounds. Laboratory tests reveal a WBC count of 18,000 with a left shift and 20 50 WBCs in the urinalysis. A CT scan of the abdomen reveals a thickened sigmoid colon with pericolonic inflammation. He is admitted to the hospital for treatment.
Which of the following is the most likely diagnosis?
A. colon cancer with contained perforation
B. ischemic colitis
C. pseudomembranous colitis
D. diverticulitis
E. pyelonephritis
Correct Answer: D
The gradual onset of left lower quadrant pain over a number of days with left lower quadrant abdominal tenderness and CT scan showing sigmoid colon inflammatory changes is most consistent with diverticulitis. Acontained perforation, either due to the diverticulitis or colon cancer, should be noted on the CT scan. There is no history of antecedent antibiotic therapy to suggest the diagnosis of pseudomembranous colitis. Though WBCs were present in the urinalysis, a diagnosis of pyelonephritis cannot be made on this basis alone, because pericolonic inflammation may be responsible for the WBCs. CT scanning is very accurate in diagnosing diverticulitis, so there is no need for any additional test. Barium enema and colonoscopy should not be performed in patients with suspected acute diverticulitis. The increased intraluminal pressure from either of these examinations may lead to free rupture of a contained abscess or phlegmon, leading to emergency surgery. However, either examination, or both, should be performed after complete resolution of diverticulitis (e.g., in 6 weeks' time) to evaluate for extent of disease, complications, and carcinoma. IVP and angiography are not indicated for diverticulitis. The appropriate management in this patient with his first episode of diverticulitis is medical management with IV antibiotics for gram- negative and anaerobic bacteria. Colon resection, either immediate or elective, should not be undertaken unless the patient's condition deteriorates or recurs. Bowel preparation cannot be performed safely in patients with acute diverticulitis. Anticoagulation has no role in therapy. Metronidazole or vancomycin therapy would be appropriate for pseudomembranous colitis, but not for diverticulitis.
Question 134:
A55-year-old man presents to the physician's office for his yearly physical examination. He is asymptomatic. Past history is pertinent for hypertension. Family history is positive for breast cancer in his mother at age 70 and colon cancer in his father at age 65. His examination is unremarkable except for guiac positive stool. Barium enema shows a sigmoid colon polyp. Colonoscopy confirms a 3-cm pedunculated polyp in the sigmoid colon, and snare polypectomy is performed. Pathologic examination reveals an adenomatous polyp with a focus of invasive carcinoma in the head, with a 4-mm resection margin and no tumor noted in the stalk. Which of the following is the most appropriate next step in management?
A. CT scan
B. magnetic resonance imaging (MRI) scan
C. surgical resection of sigmoid
D. observation
E. regular use of nonsteroidal anti-inflammatory drugs (NSAIDs)
Correct Answer: D
The prevalence of adenomas without symptoms in patients over the age of 50 ranges between 20 and 40% . Screening studies suggest that 30% of patients without symptoms over the age of 50 who undergo colonoscopy for evaluation of positive fecal occult blood have a polyp detected. Polyps greater than 2 cm have a high potential for malignant degeneration. The polyp should be completely removed, preferably by snare polypectomy. Most studies indicate that polypectomy is adequate for polyps with carcinoma in the head if the margin of resection is 2 mm or greater, especially if the stalk is not invaded. Following adequate polypectomy, observation would be indicated with postpolypectomy colonoscopic surveillance. If cancer is present at or near the margin, then colon resection is indicated. Because the incidence of residual cancer and metastatic disease is very low after successful polypectomy, scanning by CT or MRI is not indicated. The data on NSAID use are promising but insufficient to support a clinical recommendation.
Question 135:
A 65-year-old woman presents to the physician's office with a 6-month history of epigastric discomfort, poor appetite, and 10-lb weight loss. Past history is pertinent for hypertension, diabetes, a 30 pack-year smoking history, and occasional alcohol intake. Examination is unremarkable except for mild epigastric tenderness to deep palpation. An abdominal ultrasound reveals cholelithiasis, and one view of a UGI x-ray series is shown in the figure.
Which of the following is the most appropriate next step in management?
A. H2 blockers with re-evaluation by UGI in 6 months
B. vagotomy and pyloroplasty
C. total gastrectomy
D. endoscopy
E. CT scan
Correct Answer: D
The symptoms of gastric cancer are nonspecific and may mimic those of such benign conditions as benign gastric ulcer. Pain, nausea, anorexia, and weight loss are common nonspecific symptoms. A UGI series shows a gastric ulcer that has characteristics of malignancy, including an intraluminal crater with nodular margins. Agastric diverticulum would extend as a protrusion beyond the gastric lumen. The duodenum is not well visualized in the x-ray, making the diagnosis of duodenal disease difficult. Afistula would be suggested by contrast filling of the gallbladder and biliary tree. Given the x-ray findings suggestive of malignancy, the next step would be to obtain a tissue diagnosis for confirmation by endoscopy. Once malignancy is confirmed, a CT scan would be helpful to evaluate for liver metastasis and extent of disease. Operative intervention may be determined at that time, usually a subtotal or total gastrectomy. Vagotomy and pyloroplasty would not be appropriate for gastric cancer. Medical therapy with H2 blockers may improve the patient's symptoms but should not delay endoscopy and biopsy
Question 136:
A 65-year-old woman presents to the physician's office with a 6-month history of epigastric discomfort, poor appetite, and 10-lb weight loss. Past history is pertinent for hypertension, diabetes, a 30 pack-year smoking history, and occasional alcohol intake. Examination is unremarkable except for mild epigastric tenderness to deep palpation. An abdominal ultrasound reveals cholelithiasis, and one view of a UGI x-ray series is shown in the figure.
Which of the following is the most likely diagnosis?
A. cholecystoenteric fistula
B. duodenal ulcer
C. gastric ulcer
D. gastric diverticulum
E. duodenal diverticulum
Correct Answer: C
The symptoms of gastric cancer are nonspecific and may mimic those of such benign conditions as benign gastric ulcer. Pain, nausea, anorexia, and weight loss are common nonspecific symptoms. A UGI series shows a gastric ulcer that has characteristics of malignancy, including an intraluminal crater with nodular margins. Agastric diverticulum would extend as a protrusion beyond the gastric lumen. The duodenum is not well visualized in the x-ray, making the diagnosis of duodenal disease difficult. Afistula would be suggested by contrast filling of the gallbladder and biliary tree. Given the x-ray findings suggestive of malignancy, the next step would be to obtain a tissue diagnosis for confirmation by endoscopy. Once malignancy is confirmed, a CT scan would be helpful to evaluate for liver metastasis and extent of disease. Operative intervention may be determined at that time, usually a subtotal or total gastrectomy. Vagotomy and pyloroplasty would not be appropriate for gastric cancer. Medical therapy with H2 blockers may improve the patient's symptoms but should not delay endoscopy and biopsy.
Question 137:
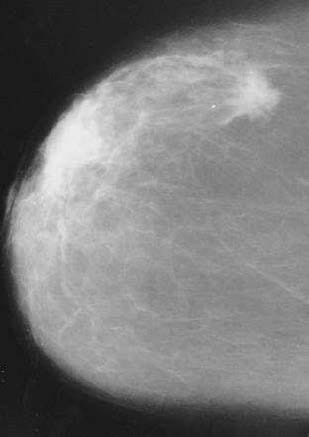
An 83-year-old woman presents to a mammographic facility for a screening mammogram. The technician notices a mass in the lateral right breast. The patient denies any breast pain, nipple discharge, skin changes, or breast trauma. A right breast CC view is shown in
Which of the following is the most appropriate next step in management?
A. incisional biopsy
B. needle biopsy
C. lumpectomy, axillary dissection, and irradiation
D. total mastectomy
E. modified radical mastectomy
Correct Answer: B
A new mass in an older woman must be evaluated for malignancy. In this case, the mammogram has characteristics of malignancy, which include a density or mass that is stellate or spiculated, irregular in size or shape, and possessing ill-defined borders. Other features suggestive of malignancy include clustered microcalcifications, asymmetric density, architectural distortion, and skin or nipple retraction. DCIS usually presents as calcifications without a definite mass. Cystosarcoma phyllodes presents much like a fibroadenoma as a well-defined mass with smooth margins. Papillomas are small and not usually palpable or noted by mammography. Fat necrosis can mimic the mammographic features of malignancy and is often associated with trauma. However, only when an oil cyst is noted, can an unequivocal diagnosis of fat necrosis be made. The next step is needle biopsy, by FNA, or core biopsy so a histologic diagnosis can be made and options for management (i.e., modified radical mastectomy or lumpectomy, axillary dissection, and irradiation) discussed. Needle biopsy is less invasive and less expensive than incisional biopsy and, therefore, is preferred. Excisional biopsy (not listed) is acceptable, but often requires a two-step procedure, the first to establish the diagnosis and the second for definitive treatment. Aneedle biopsy, especially a core biopsy that renders a histologic diagnosis, can often avoid the necessity of a second surgical procedure.
Question 138:
An 83-year-old woman presents to a mammographic facility for a screening mammogram. The technician notices a mass in the lateral right breast. The patient denies any breast pain, nipple discharge, skin changes, or breast trauma. A right breast CC view is shown in
Which of the following is the most likely diagnosis?
A. papilloma
B. invasive carcinoma
C. cystosarcoma phyllodes
D. DCIS
E. fat necrosis
Correct Answer: B
A new mass in an older woman must be evaluated for malignancy. In this case, the mammogram has characteristics of malignancy, which include a density or mass that is stellate or spiculated, irregular in size or shape, and possessing ill-defined borders. Other features suggestive of malignancy include clustered microcalcifications, asymmetric density, architectural distortion, and skin or nipple retraction. DCIS usually presents as calcifications without a definite mass. Cystosarcoma phyllodes presents much like a fibroadenoma as a well-defined mass with smooth margins. Papillomas are small and not usually palpable or noted by mammography. Fat necrosis can mimic the mammographic features of malignancy and is often associated with trauma. However, only when an oil cyst is noted, can an unequivocal diagnosis of fat necrosis be made. The next step is needle biopsy, by FNA, or core biopsy so a histologic diagnosis can be made and options for management (i.e., modified radical mastectomy or lumpectomy, axillary dissection, and irradiation) discussed. Needle biopsy is less invasive and less expensive than incisional biopsy and, therefore, is preferred. Excisional biopsy (not listed) is acceptable, but often requires a two-step procedure, the first to establish the diagnosis and the second for definitive treatment. Aneedle biopsy, especially a core biopsy that renders a histologic diagnosis, can often avoid the necessity of a second surgical procedure.
Question 139:
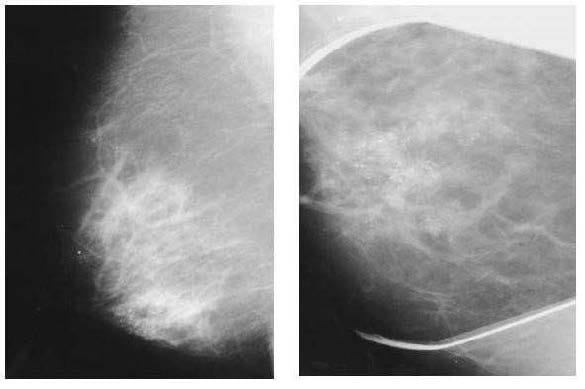
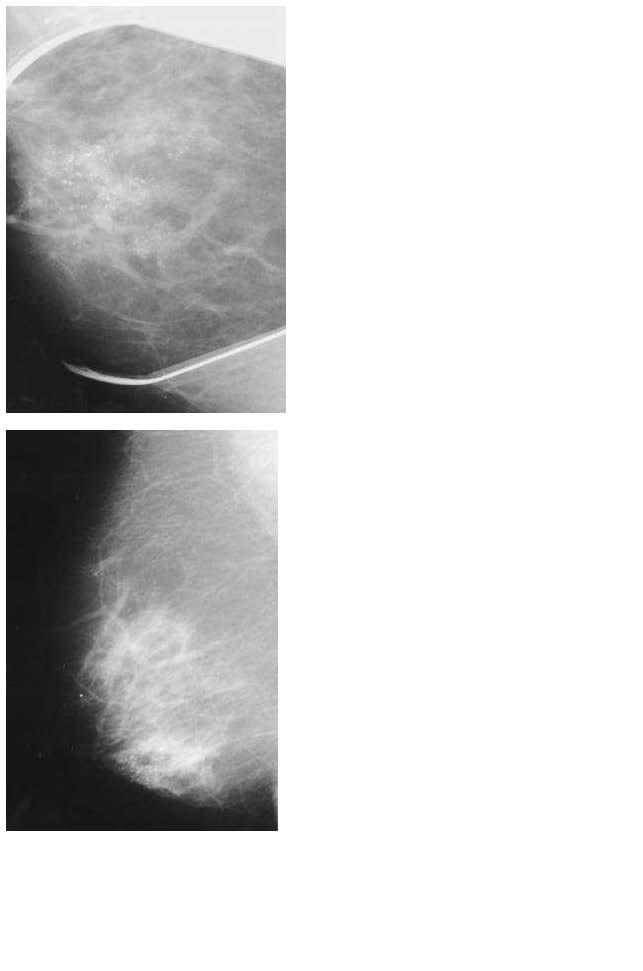
A 65-year-old woman presents to the physician's office for evaluation of an abnormal screening mammogram. She denies any breast masses, nipple discharge, pain, or skin changes. Past history is pertinent for hypertension. Family history is positive for postmenopausal breast cancer in a sister. She has a normal breast examination and no axillary adenopathy. The remainder of her examination is unremarkable. An MLO view of the right breast is shown in Figure along with a magnification view of the craniocaudal (CC) film Which of the following is the most appropriate next step in management?
A. observation, with repeat mammogram in 6 months
B. observation, with repeat mammogram on an annual basis
C. biopsy
D. lumpectomy, radiation therapy, and SLN biopsy
E. total mastectomy
Correct Answer: C
The mammographic appearance is most consistent with DCIS with or without an invasive component. The calcifications of DCIS are clustered, pleomorphic, irregular, and linear, and may be associated with a mass representing an invasive carcinoma. LCIS does not usually present with calcifications. Cystosarcoma phyllodes presents as a mass, often indistinguishable from a fibroadenoma. An involuting fibroadenoma often presents as a mass with large, coarse calcifications, indicating its benignity. Milk of calcium will often layer differently in the CC and mediolateral projections, suggesting fluid with calcium. The next step in management is to obtain a biopsy, preferably a core needle biopsy, for histologic confirmation and to evaluate for invasive disease. Observation is not recommended because these calcifications appear malignant. All other choices (i.e., lumpectomy or total mastectomy) are not indicated until a diagnosis by biopsy is obtained.
Question 140:
A 65-year-old woman presents to the physician's office for evaluation of an abnormal screening mammogram. She denies any breast masses, nipple discharge, pain, or skin changes. Past history is pertinent for hypertension. Family history is positive for postmenopausal breast cancer in a sister. She has a normal breast examination and no axillary adenopathy. The remainder of her examination is unremarkable. An MLO view of the right breast is shown in Figure along with a magnification view of the craniocaudal (CC) film
Which of the following is the most likely diagnosis?
A. milk of calcium
B. LCIS with or without an invasive component
C. DCIS with or without an invasive component
D. involuting fibroadenoma
E. phyllodes tumor
Correct Answer: C
The mammographic appearance is most consistent with DCIS with or without an invasive component. The calcifications of DCIS are clustered, pleomorphic, irregular, and linear, and may be associated with a mass representing an invasive carcinoma. LCIS does not usually present with calcifications. Cystosarcoma phyllodes presents as a mass, often indistinguishable from a fibroadenoma. An involuting fibroadenoma often presents as a mass with large, coarse calcifications, indicating its benignity. Milk of calcium will often layer differently in the CC and mediolateral projections, suggesting fluid with calcium. The next step in management is to obtain a biopsy, preferably a core needle biopsy, for histologic confirmation and to evaluate for invasive disease. Observation is not recommended because these calcifications appear malignant. All other choices (i.e., lumpectomy or total mastectomy) are not indicated until a diagnosis by biopsy is obtained.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.