A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
Of the options listed, which would be the most appropriate management at this point?
A. recommendation of a low salt diet and follow-up in 912 months
B. increasing the dosage of the previously started antihypertensive medication
C. initiating therapy with a calcium channel blocker
D. initiating therapy with a thiazide diuretic
E. initiating therapy with a thiazide diuretic and an angiotensin-converting enzyme (ACE) inhibitor
Correct Answer: E Section: (none)
Explanation: Explanations: The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) was released in May, 2003. It provides evidence-based guidelines for the detection, evaluation, and treatment of hypertension, the most common primary diagnosis in the United States. One of the key guidelines presented in this report is the classification of blood pressure for adults. The classification is based on the average of two or more properly measured, seated, blood pressure readings on each of two or more office visits. The proper measurement of blood pressure is critical. Blood pressure should be measured using a properly calibrated instrument in a patient who has been seated quietly in a chair for at least 5 minutes, with his feet on the floor and arm supported at heart level. The blood pressure cuff should encircle at least 80% of the arm. The systolic blood pressure is the point at which the first of two or more sounds is heard and the diastolic blood pressure is the point before the sounds disappear. In question 10, where an incidentally noted elevated blood pressure reading is found, it is then necessary to perform blood pressure measurements following the JNC 7 guidelines--two or more readings after the patient has been seated quietly in a chair for 5 or more minutes. Institution of antihypertensive medications would be inappropriate based on one blood pressure reading in this range, as the patient has not been diagnosed as hypertensive as of yet. Aspirin therapy is recommended for most persons over the age of 50 for the primary prevention of CHD events and would be recommended for others at high risk of heart disease.
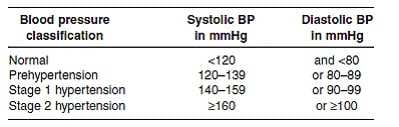
In persons with hypertension, it is recommended to start aspirin after their blood pressure is controlled because the risk of hemorrhagic stroke is increased in uncontrolled hypertension. Risk stratification with an exercise stress test at this point is not supported by evidence showing a reduction of morbidity or mortality and is likely to have many false positive results. Discontinuation of his nasal steroid is unnecessary as it is unlikely to be affecting his blood pressure adversely and should provide good symptomatic relief of his seasonal allergy symptoms. The blood pressure classifications from the JNC 7 report are as follows:
This classification regimen represents a change from previous JNC guidelines with the designation of a prehypertension classification and the combination of the previous stage 2 and stage 3 into a single stage 2 category. By this categorization, the patient in this question has stage 2 hypertension. Recommended evaluation of patients with hypertension includes an ECG, measurement of blood glucose, hematocrit, serum potassium, creatinine and calcium, urinalysis, and a fasting lipid profile. Other testing is not indicated unless suggested by the presence of symptoms or if blood pressure control cannot be achieved. The management of hypertension involves the institution of lifestyle recommendations and, frequently, the use of antihypertensive medications. Lifestyle modifications can lower blood pressure, enhance the effectiveness of medications, and reduce cardiovascular risks. A low salt diet by itself may lower systolic blood pressure by 28 mmHg and is not likely to bring this patient to a goal blood pressure if that is the only modification made. Other lifestyle modifications, including the DASH (dietary approaches to stop hypertension) eating plan and increasing physical
Question 182:
A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
Further evaluation at this point should include which of these?
A. 24-hour urine collection for protein and creatinine clearance
B. renal artery Doppler studies to evaluate for renal artery stenosis C. an ECG
C. an echocardiogram to evaluate for ventricular hypertrophy
D. a serum measurement of thyroidstimulating hormone (TSH)
Correct Answer: C Section: (none)
Explanation: Explanations: The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) was released in May, 2003. It provides evidence-based guidelines for the detection, evaluation, and treatment of hypertension, the most common primary diagnosis in the United States. One of the key guidelines presented in this report is the classification of blood pressure for adults. The classification is based on the average of two or more properly measured, seated, blood pressure readings on each of two or more office visits. The proper measurement of blood pressure is critical. Blood pressure should be measured using a properly calibrated instrument in a patient who has been seated quietly in a chair for at least 5 minutes, with his feet on the floor and arm supported at heart level. The blood pressure cuff should encircle at least 80% of the arm. The systolic blood pressure is the point at which the first of two or more sounds is heard and the diastolic blood pressure is the point before the sounds disappear. In question 10, where an incidentally noted elevated blood pressure reading is found, it is then necessary to perform blood pressure measurements following the JNC 7 guidelines--two or more readings after the patient has been seated quietly in a chair for 5 or more minutes. Institution of antihypertensive medications would be inappropriate based on one blood pressure reading in this range, as the patient has not been diagnosed as hypertensive as of yet. Aspirin therapy is recommended for most persons over the age of 50 for the primary prevention of CHD events and would be recommended for others at high risk of heart disease.
In persons with hypertension, it is recommended to start aspirin after their blood pressure is controlled because the risk of hemorrhagic stroke is increased in uncontrolled hypertension. Risk stratification with an exercise stress test at this point is not supported by evidence showing a reduction of morbidity or mortality and is likely to have many false positive results. Discontinuation of his nasal steroid is unnecessary as it is unlikely to be affecting his blood pressure adversely and should provide good symptomatic relief of his seasonal allergy symptoms. The blood pressure classifications from the JNC 7 report are as follows:
This classification regimen represents a change from previous JNC guidelines with the designation of a prehypertension classification and the combination of the previous stage 2 and stage 3 into a single stage 2 category. By this categorization, the patient in this question has stage 2 hypertension. Recommended evaluation of patients with hypertension includes an ECG, measurement of blood glucose, hematocrit, serum potassium, creatinine and calcium, urinalysis, and a fasting lipid profile. Other testing is not indicated unless suggested by the presence of symptoms or if blood pressure control cannot be achieved. The management of hypertension involves the institution of lifestyle recommendations and, frequently, the use of antihypertensive medications. Lifestyle modifications can lower blood pressure, enhance the effectiveness of medications, and reduce cardiovascular risks. A low salt diet by itself may lower systolic blood pressure by 28 mmHg and is not likely to bring this patient to a goal blood pressure if that is the only modification made. Other lifestyle modifications, including the DASH (dietary approaches to stop hypertension) eating plan and increasing physical
Question 183:
A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
The patient returns for a follow-up visit and his blood pressure is 165/105 mmHg. You diagnose him with which of the following?
A. elevated blood pressure without hypertension
B. prehypertension
C. stage 1 hypertension
D. stage 2 hypertension
E. stage 3 hypertension
Correct Answer: D Section: (none)
Explanation: Explanations: The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) was released in May, 2003. It provides evidence-based guidelines for the detection, evaluation, and treatment of hypertension, the most common primary diagnosis in the United States. One of the key guidelines presented in this report is the classification of blood pressure for adults. The classification is based on the average of two or more properly measured, seated, blood pressure readings on each of two or more office visits. The proper measurement of blood pressure is critical. Blood pressure should be measured using a properly calibrated instrument in a patient who has been seated quietly in a chair for at least 5 minutes, with his feet on the floor and arm supported at heart level. The blood pressure cuff should encircle at least 80% of the arm. The systolic blood pressure is the point at which the first of two or more sounds is heard and the diastolic blood pressure is the point before the sounds disappear. In question 10, where an incidentally noted elevated blood pressure reading is found, it is then necessary to perform blood pressure measurements following the JNC 7 guidelines--two or more readings after the patient has been seated quietly in a chair for 5 or more minutes. Institution of antihypertensive medications would be inappropriate based on one blood pressure reading in this range, as the patient has not been diagnosed as hypertensive as of yet. Aspirin therapy is recommended for most persons over the age of 50 for the primary prevention of CHD events and would be recommended for others at high risk of heart disease.
In persons with hypertension, it is recommended to start aspirin after their blood pressure is controlled because the risk of hemorrhagic stroke is increased in uncontrolled hypertension. Risk stratification with an exercise stress test at this point is not supported by evidence showing a reduction of morbidity or mortality and is likely to have many false positive results. Discontinuation of his nasal steroid is unnecessary as it is unlikely to be affecting his blood pressure adversely and should provide good symptomatic relief of his seasonal allergy symptoms. The blood pressure classifications from the JNC 7 report are as follows:
This classification regimen represents a change from previous JNC guidelines with the designation of a prehypertension classification and the combination of the previous stage 2 and stage 3 into a single stage 2 category. By this categorization, the patient in this question has stage 2 hypertension. Recommended evaluation of patients with hypertension includes an ECG, measurement of blood glucose, hematocrit, serum potassium, creatinine and calcium, urinalysis, and a fasting lipid profile. Other testing is not indicated unless suggested by the presence of symptoms or if blood pressure control cannot be achieved. The management of hypertension involves the institution of lifestyle recommendations and, frequently, the use of antihypertensive medications. Lifestyle modifications can lower blood pressure, enhance the effectiveness of medications, and reduce cardiovascular risks. A low salt diet by itself may lower systolic blood pressure by 28 mmHg and is not likely to bring this patient to a goal blood pressure if that is the only modification made. Other lifestyle modifications, including the DASH (dietary approaches to stop hypertension) eating plan and increasing physical
Question 184:
A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
Initial management at this time should include which of the following?
A. institution of therapy with a betablocker or thiazide diuretic
B. repeat blood pressure in each arm after he sits quietly for 5 minutes
C. recommendation to start taking a baby aspirin a day
D. a treadmill exercise stress test to stratify his risk for coronary artery disease
E. discontinuation of his nasal steroid
Correct Answer: B Section: (none)
Explanation: Explanations: The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) was released in May, 2003. It provides evidence-based guidelines for the detection, evaluation, and treatment of hypertension, the most common primary diagnosis in the United States. One of the key guidelines presented in this report is the classification of blood pressure for adults. The classification is based on the average of two or more properly measured, seated, blood pressure readings on each of two or more office visits. The proper measurement of blood pressure is critical. Blood pressure should be measured using a properly calibrated instrument in a patient who has been seated quietly in a chair for at least 5 minutes, with his feet on the floor and arm supported at heart level. The blood pressure cuff should encircle at least 80% of the arm. The systolic blood pressure is the point at which the first of two or more sounds is heard and the diastolic blood pressure is the point before the sounds disappear. In question 10, where an incidentally noted elevated blood pressure reading is found, it is then necessary to perform blood pressure measurements following the JNC 7 guidelines--two or more readings after the patient has been seated quietly in a chair for 5 or more minutes. Institution of antihypertensive medications would be inappropriate based on one blood pressure reading in this range, as the patient has not been diagnosed as hypertensive as of yet. Aspirin therapy is recommended for most persons over the age of 50 for the primary prevention of CHD events and would be recommended for others at high risk of heart disease.
In persons with hypertension, it is recommended to start aspirin after their blood pressure is controlled because the risk of hemorrhagic stroke is increased in uncontrolled hypertension. Risk stratification with an exercise stress test at this point is not supported by evidence showing a reduction of morbidity or mortality and is likely to have many false positive results. Discontinuation of his nasal steroid is unnecessary as it is unlikely to be affecting his blood pressure adversely and should provide good symptomatic relief of his seasonal allergy symptoms. The blood pressure classifications from the JNC 7 report are as follows: This classification regimen represents a change from previous JNC guidelines with the designation of a prehypertension classification and the combination of the previous stage 2 and stage 3 into a single stage 2 category. By this categorization, the patient in this question has stage 2 hypertension. Recommended evaluation of patients with hypertension includes an ECG, measurement of blood glucose, hematocrit, serum potassium, creatinine and calcium, urinalysis, and a fasting lipid profile. Other testing is not indicated unless suggested by the presence of symptoms or if blood pressure control cannot be achieved. The management of hypertension involves the institution of lifestyle recommendations and, frequently, the use of antihypertensive medications. Lifestyle modifications can lower blood pressure, enhance the effectiveness of medications, and reduce cardiovascular risks. A low salt diet by itself may lower systolic blood pressure by 28 mmHg and is not likely to bring this patient to a goal blood pressure if that is the only modification made. Other lifestyle modifications, including the DASH (dietary approaches to stop hypertension) eating plan and increasing physical
Question 185:
A 40-year-old male comes to your office as a new patient to get established for care, as he recently moved into your city from another state. He has been on medical therapy for type 2 diabetes mellitus for 3 years and has had good glycemic control. He takes metformin 500 mg bid and reports having fasting glucose levels of less than 100 on home monitoring. He has records from his previous physician that show that he had a dilated eye examination 6 months ago that was normal and a hemoglobin A1C (HgbA1C) level of 6.2 that was taken 3 months ago. He has no known history of coronary artery disease. His last fasting lipid measurement was 14 months ago. You order a fasting lipid panel today and get the following results:
He states that he has not had any immunizations in "longer than I can remember." Which of the following would be recommended for him?
A. hepatitis A and hepatitis B vaccines
B. herpes zoster vaccine (Zostavax)
C. tetanus, diphtheria, and acellular pertussis (Tdap) vaccine
D. tetanus and diphtheria (Td) vaccine
E. Tdap and PPV-23
Correct Answer: E Section: (none)
Explanation: Explanations: The Third Report of the National Cholesterol Education Program Expert Panel on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) was published in May 2001 by the National Heart, Lung, and Blood Institute of the National Institutes of Health. This evidence-based report provides guidelines for the evaluation and management of blood lipid levels for the primary and secondary prevention of heart disease. The basis of the recommendations for management is an overall evaluation of an individual's risk factors for developing cardiovascular disease. Persons at the highest risk for future cardiac events are those with already established coronary artery disease or "coronary artery disease equivalents," which include diabetes mellitus, other forms of atherosclerotic disease, or multiple risk factors that confer a 10-year CHD risk of greater than 20%. Multiple studies have shown that elevated LDL cholesterol levels are a risk for coronary artery disease and that lowering LDL levels can reduce the risk of events.
ATP III goals are targeted at LDL levels. For persons with LDL levels above this goal, the options for lowering LDL can include therapeutic lifestyle changes, lipid-lowering medications, or a combination of both. In a patient with coronary artery disease, diabetes mellitus, or other CHD equivalents, the LDL goal level is 100 mg/dL. In this population, therapeutic lifestyle changes alone would be recommended for those with LDL levels of 100130 and medication could be started concomitantly with lifestyle changes for those with LDL above 130, as most persons would require medication to achieve the recommended goal. For the patient in this question with an LDL of 160 mg/dL, therapy with an HMG-CoA reductase inhibitor would be recommended first-line therapy to try to get his LDLto goal. Therapeutic lifestyle changes alone would be very unlikely to reduce his LDL to less than 100 mg/dL, but are still an important part of his overall lipid management program and should be recommended along with medication therapy. Neither increasing his dosage of metformin nor adding insulin would be recommended as they would not be expected to improve his dyslipidemia significantly and because his diabetic control is appropriate. At his follow-up visit, the patient's lipid levels have met the recommended guidelines; therefore, the recommendation would be to continue with his current therapy. Increasing the dosage of his statin, adding a fibric acid, nicotinic acid, or referring the patient to a dietician would all be appropriate considerations in someone who had not successfully reached his goal lipid levels.
A recent addition to the ATP III provides an option for changing the target LDL goal for those at the highest of risk for coronary events. For persons with known coronary artery disease, or CAD equivalent, and multiple risk factors, such as diabetes or continued smoking, one could consider using an LDL of 70 as a goal. For this patient, with diabetes but no history of CAD or equivalent, the recommended goal would remain an LDL of 100 or less. Immunizations should be a routine part of the adult health maintenance evaluation. All patients with diabetes are recommended to be vaccinated with the pneumococcal vaccine (PPV-23) both because of the incidence of pneumonia in diabetics and the increased risk of complications should infection occur. A recent recommendation for all adults is to provide a single dose of Tdap vaccine in place of one booster dose of Td. The rationale for this is to attempt to reduce the incidence of pertussis in the population, as pertussis has been recurring in the United States in spite of routine childhood vaccination. Hepatitis A and B are routine vaccinations for children. The current recommendation for adult immunizations against these diseases is to target high-risk adults. Diabetes is not considered a high risk for these infections. Herpes zoster vaccine is recommended for adults over the age of 60
Question 186:
A 40-year-old male comes to your office as a new patient to get established for care, as he recently moved into your city from another state. He has been on medical therapy for type 2 diabetes mellitus for 3 years and has had good glycemic control. He takes metformin 500 mg bid and reports having fasting glucose levels of less than 100 on home monitoring. He has records from his previous physician that show that he had a dilated eye examination 6 months ago that was normal and a hemoglobin A1C (HgbA1C) level of 6.2 that was taken 3 months ago. He has no known history of coronary artery disease. His last fasting lipid measurement was 14 months ago. You order a fasting lipid panel today and get the following results:
Your recommendations for today include which of the following?
A. continue his current regimen without change
B. add nicotinic acid
C. add a fibric acid
D. refer the patient to a dietician for counseling
E. increase the dosage of his HMG-CoA reductase inhibitor
Correct Answer: A Section: (none)
Explanation: Explanations: The Third Report of the National Cholesterol Education Program Expert Panel on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) was published in May 2001 by the National Heart, Lung, and Blood Institute of the National Institutes of Health. This evidence-based report provides guidelines for the evaluation and management of blood lipid levels for the primary and secondary prevention of heart disease. The basis of the recommendations for management is an overall evaluation of an individual's risk factors for developing cardiovascular disease. Persons at the highest risk for future cardiac events are those with already established coronary artery disease or "coronary artery disease equivalents," which include diabetes mellitus, other forms of atherosclerotic disease, or multiple risk factors that confer a 10-year CHD risk of greater than 20%. Multiple studies have shown that elevated LDL cholesterol levels are a risk for coronary artery disease and that lowering LDL levels can reduce the risk of events. ATP III goals are targeted at LDL levels. For persons with LDL levels above this goal, the options for lowering LDL can include therapeutic lifestyle changes, lipid-lowering medications, or a combination of both. In a patient with coronary artery disease, diabetes mellitus, or other CHD equivalents, the LDL goal level is 100 mg/dL. In this population, therapeutic lifestyle changes alone would be recommended for those with LDL levels of 100130 and medication could be started concomitantly with lifestyle changes for those with LDL above 130, as most persons would require medication to achieve the recommended goal. For the patient in this question with an LDL of 160 mg/dL, therapy with an HMG-CoA reductase inhibitor would be recommended first-line therapy to try to get his LDLto goal. Therapeutic lifestyle changes alone would be very unlikely to reduce his LDL to less than 100 mg/dL, but are still an important part of his overall lipid management program and should be recommended along with medication therapy. Neither increasing his dosage of metformin nor adding insulin would be recommended as they would not be expected to improve his dyslipidemia significantly and because his diabetic control is appropriate. At his follow-up visit, the patient's lipid levels have met the recommended guidelines; therefore, the recommendation would be to continue with his current therapy. Increasing the dosage of his statin, adding a fibric acid, nicotinic acid, or referring the patient to a dietician would all be appropriate considerations in someone who had not successfully reached his goal lipid levels.
A recent addition to the ATP III provides an option for changing the target LDL goal for those at the highest of risk for coronary events. For persons with known coronary artery disease, or CAD equivalent, and multiple risk factors, such as diabetes or continued smoking, one could consider using an LDL of 70 as a goal. For this patient, with diabetes but no history of CAD or equivalent, the recommended goal would remain an LDL of 100 or less. Immunizations should be a routine part of the adult health maintenance evaluation. All patients with diabetes are recommended to be vaccinated with the pneumococcal vaccine (PPV-23) both because of the incidence of pneumonia in diabetics and the increased risk of complications should infection occur. A recent recommendation for all adults is to provide a single dose of Tdap vaccine in place of one booster dose of Td. The rationale for this is to attempt to reduce the incidence of pertussis in the population, as pertussis has been recurring in the United States in spite of routine childhood vaccination. Hepatitis A and B are routine vaccinations for children. The current recommendation for adult immunizations against these diseases is to target high-risk adults. Diabetes is not considered a high risk for these infections. Herpes zoster vaccine is recommended for adults over the age of 60
Question 187:
A 40-year-old male comes to your office as a new patient to get established for care, as he recently moved into your city from another state. He has been on medical therapy for type 2 diabetes mellitus for 3 years and has had good glycemic control. He takes metformin 500 mg bid and reports having fasting glucose levels of less than 100 on home monitoring. He has records from his previous physician that show that he had a dilated eye examination 6 months ago that was normal and a hemoglobin A1C (HgbA1C) level of 6.2 that was taken 3 months ago. He has no known history of coronary artery disease. His last fasting lipid measurement was 14 months ago. You order a fasting lipid panel today and get the following results:
Your management today should include which of the following?
A. institution of a low-carbohydrate diet
B. increasing his dosage of metformin
C. starting the patient on insulin therapy
D. continuing his current care without change
E. starting the patient on a hydroxymethylglutaryl-coenzyme A (HMG-CoA) reductase inhibitor (statin)
Correct Answer: E Section: (none)
Explanation: Explanations: The Third Report of the National Cholesterol Education Program Expert Panel on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) was published in May 2001 by the National Heart, Lung, and Blood Institute of the National Institutes of Health. This evidence-based report provides guidelines for the evaluation and management of blood lipid levels for the primary and secondary prevention of heart disease. The basis of the recommendations for management is an overall evaluation of an individual's risk factors for developing cardiovascular disease. Persons at the highest risk for future cardiac events are those with already established coronary artery disease or "coronary artery disease equivalents," which include diabetes mellitus, other forms of atherosclerotic disease, or multiple risk factors that confer a 10-year CHD risk of greater than 20%. Multiple studies have shown that elevated LDL cholesterol levels are a risk for coronary artery disease and that lowering LDL levels can reduce the risk of events.
ATP III goals are targeted at LDL levels. For persons with LDL levels above this goal, the options for lowering LDL can include therapeutic lifestyle changes, lipid-lowering medications, or a combination of both. In a patient with coronary artery disease, diabetes mellitus, or other CHD equivalents, the LDL goal level is 100 mg/dL. In this population, therapeutic lifestyle changes alone would be recommended for those with LDL levels of 100130 and medication could be started concomitantly with lifestyle changes for those with LDL above 130, as most persons would require medication to achieve the recommended goal. For the patient in this question with an LDL of 160 mg/dL, therapy with an HMG-CoA reductase inhibitor would be recommended first-line therapy to try to get his LDLto goal. Therapeutic lifestyle changes alone would be very unlikely to reduce his LDL to less than 100 mg/dL, but are still an important part of his overall lipid management program and should be recommended along with medication therapy. Neither increasing his dosage of metformin nor adding insulin would be recommended as they would not be expected to improve his dyslipidemia significantly and because his diabetic control is appropriate. At his follow-up visit, the patient's lipid levels have met the recommended guidelines; therefore, the recommendation would be to continue with his current therapy. Increasing the dosage of his statin, adding a fibric acid, nicotinic acid, or referring the patient to a dietician would all be appropriate considerations in someone who had not successfully reached his goal lipid levels.
A recent addition to the ATP III provides an option for changing the target LDL goal for those at the highest of risk for coronary events. For persons with known coronary artery disease, or CAD equivalent, and multiple risk factors, such as diabetes or continued smoking, one could consider using an LDL of 70 as a goal. For this patient, with diabetes but no history of CAD or equivalent, the recommended goal would remain an LDL of 100 or less. Immunizations should be a routine part of the adult health maintenance evaluation. All patients with diabetes are recommended to be vaccinated with the pneumococcal vaccine (PPV-23) both because of the incidence of pneumonia in diabetics and the increased risk of complications should infection occur. A recent recommendation for all adults is to provide a single dose of Tdap vaccine in place of one booster dose of Td. The rationale for this is to attempt to reduce the incidence of pertussis in the population, as pertussis has been recurring in the United States in spite of routine childhood vaccination. Hepatitis A and B are routine vaccinations for children. The current recommendation for adult immunizations against these diseases is to target high-risk adults. Diabetes is not considered a high risk for these infections. Herpes zoster vaccine is recommended for adults over the age of 60
Question 188:
A65-year-old White female presents to the office for her annual gynecologic examination. She has been a patient of yours for many years. She also sees you on a routine basis for treatment of hypertension and hypothyroidism. Her last pap smear was 5 years ago and she has never had an abnormal pap smear. She had a mammogram 1 year ago that was normal. She does not perform self-breast examination. She is without complaint today.
Past medical 1. Hypertension for 15 years history: 2. Graves' disease, treated with radioactive iodine thyroid ablation at age 50 OB/GYN history: 1. Menarche at age 14
2.
Four term pregnancies with vaginal deliveries (at age 22, 25, 27, and 32)
3.
Total abdominal hysterectomy and bilateral salpingo oophorectomy (TAH/BSO) age 47 for fibroids
4.
On estrogen replacement therapy from age 47 to 55 Past surgical 1. Appendectomy at age 16 history:
Potassium chloride 20 meq daily Allergies: None Family history: Parents, siblings unknown as patient was adopted Children are alive and well without known chronic medical conditions Social history: Widowed for 5 years, has not been involved in a sexual relationship since the death of her husband; retired school teacher; college educated; does not smoke cigarettes, drink alcohol, or use drugs; walks 3045 min a day for exercise
Which of the following vaccinations would be routinely recommended for this patient?
A. hepatitis B vaccine
B. measles, mumps, rubella (MMR) if patient does not recall having the measles
C. pneumococcal conjugate vaccine (PCV-7)
D. pneumococcal polysaccharide vaccine (PPV-23)
E. hepatitis A vaccine
Correct Answer: D Section: (none)
Explanation: Explanations: Screening for osteoporosis in women 65 years old or older is a level B recommendation of the USPSTF, as detection and treatment of osteoporosis may reduce fracture risk. In women who have had a hysterectomy (with removal of the cervix) for reasons other than cervical cancer, pap smear screening of the vaginal cuff is not recommended and cytologic screening can be discontinued. Therapy with either estrogen alone (in women who do not have a uterus) or combined estrogen and progesterone (in women who have a uterus) in postmenopausal women is controversial. Based on findings of the Women's Health Initiative and other studies, the USPSTF gives a level D recommendation to the use of combined estrogen and progesterone therapy and level I recommendation for estrogen therapy alone for the prevention of chronic conditions. Screening for asymptomatic bacteruria in all populations other than pregnant women is given a level D recommendation. No benefit from the intervention has been found and overtreatment with antibiotics may produce harm. While mammography for breast cancer screening has been given a level B recommendation, both self-breast examination and clinical breast examination are level I recommendations, with insufficient evidence to show any benefit in morbidity or mortality.
According to the Centers for Disease Control, diseases of the heart make up the most common cause of death in women in this age group. Heart disease is responsible for approximately one-third of all deaths in women aged 65 and older. Malignant neoplasms make up the next largest cause of death, followed by cerebrovascular diseases and chronic lower respiratory diseases. PPV-23 is recommended for all adults over the age of 65 and at younger ages for individuals at high risk for pneumonia or complications of pneumonia. These include persons with diabetes mellitus, chronic obstructive pulmonary disease, coronary artery disease, and those who have had a splenectomy or are functionally asplenic. The PCV-7 is recommended for the routine vaccination of children. Hepatitis B vaccine is recommended universally for children and for adults who are at high risk for the disease based on profession or lifestyle. Hepatitis A vaccine is recommended for children who live in certain areas of the United States in which the disease is prevalent and may be offered electively to persons traveling to endemic areas. The MMR vaccine is recommended to all children but is not indicated in adults. Rubella vaccination is recommended for women of childbearing age who may become pregnant and who do not have immunity to rubella, in an effort to reduce the risk of congenital rubella infection
Question 189:
A65-year-old White female presents to the office for her annual gynecologic examination. She has been a patient of yours for many years. She also sees you on a routine basis for treatment of hypertension and hypothyroidism. Her last pap smear was 5 years ago and she has never had an abnormal pap smear. She had a mammogram 1 year ago that was normal. She does not perform self-breast examination. She is without complaint today.
Past medical 1. Hypertension for 15 years history: 2. Graves' disease, treated with radioactive iodine thyroid ablation at age 50 OB/GYN history: 1. Menarche at age 14
2.
Four term pregnancies with vaginal deliveries (at age 22, 25, 27, and 32)
3.
Total abdominal hysterectomy and bilateral salpingo oophorectomy (TAH/BSO) age 47 for fibroids
4.
On estrogen replacement therapy from age 47 to 55 Past surgical 1. Appendectomy at age 16 history:
Potassium chloride 20 meq daily Allergies: None Family history: Parents, siblings unknown as patient was adopted Children are alive and well without known chronic medical conditions Social history: Widowed for 5 years, has not been involved in a sexual relationship since the death of her husband; retired school teacher; college educated; does not smoke cigarettes, drink alcohol, or use drugs; walks 3045 min a day for exercise
Which of the following conditions results in the most deaths of American women over the age of 65?
A. breast cancer
B. ovarian cancer
C. lung cancer
D. cardiovascular disease
E. pneumonia
Correct Answer: D Section: (none)
Explanation: Explanations: Screening for osteoporosis in women 65 years old or older is a level B recommendation of the USPSTF, as detection and treatment of osteoporosis may reduce fracture risk. In women who have had a hysterectomy (with removal of the cervix) for reasons other than cervical cancer, pap smear screening of the vaginal cuff is not recommended and cytologic screening can be discontinued. Therapy with either estrogen alone (in women who do not have a uterus) or combined estrogen and progesterone (in women who have a uterus) in postmenopausal women is controversial. Based on findings of the Women's Health Initiative and other studies, the USPSTF gives a level D recommendation to the use of combined estrogen and progesterone therapy and level I recommendation for estrogen therapy alone for the prevention of chronic conditions. Screening for asymptomatic bacteruria in all populations other than pregnant women is given a level D recommendation. No benefit from the intervention has been found and overtreatment with antibiotics may produce harm. While mammography for breast cancer screening has been given a level B recommendation, both self-breast examination and clinical breast examination are level I recommendations, with insufficient evidence to show any benefit in morbidity or mortality. According to the Centers for Disease Control, diseases of the heart make up the most common cause of death in women in this age group. Heart disease is responsible for approximately one-third of all deaths in women aged 65 and older. Malignant neoplasms make up the next largest cause of death, followed by cerebrovascular diseases and chronic lower respiratory diseases. PPV-23 is recommended for all adults over the age of 65 and at younger ages for individuals at high risk for pneumonia or complications of pneumonia. These include persons with diabetes mellitus, chronic obstructive pulmonary disease, coronary artery disease, and those who have had a splenectomy or are functionally asplenic. The PCV-7 is recommended for the routine vaccination of children. Hepatitis B vaccine is recommended universally for children and for adults who are at high risk for the disease based on profession or lifestyle. Hepatitis A vaccine is recommended for children who live in certain areas of the United States in which the disease is prevalent and may be offered electively to persons traveling to endemic areas. The MMR vaccine is recommended to all children but is not indicated in adults. Rubella vaccination is recommended for women of childbearing age who may become pregnant and who do not have immunity to rubella, in an effort to reduce the risk of congenital rubella infection
Question 190:
A65-year-old White female presents to the office for her annual gynecologic examination. She has been a patient of yours for many years. She also sees you on a routine basis for treatment of hypertension and hypothyroidism. Her last pap smear was 5 years ago and she has never had an abnormal pap smear. She had a mammogram 1 year ago that was normal. She does not perform self-breast examination. She is without complaint today.
Past medical 1. Hypertension for 15 years history: 2. Graves' disease, treated with radioactive iodine thyroid ablation at age 50 OB/GYN history: 1. Menarche at age 14
2.
Four term pregnancies with vaginal deliveries (at age 22, 25, 27, and 32)
3.
Total abdominal hysterectomy and bilateral salpingo oophorectomy (TAH/BSO) age 47 for fibroids
4.
On estrogen replacement therapy from age 47 to 55 Past surgical 1. Appendectomy at age 16 history:
Potassium chloride 20 meq daily Allergies: None Family history: Parents, siblings unknown as patient was adopted Children are alive and well without known chronic medical conditions Social history: Widowed for 5 years, has not been involved in a sexual relationship since the death of her husband; retired school teacher; college educated; does not smoke cigarettes, drink alcohol, or use drugs; walks 3045 min a day for exercise
At this visit you should do which of the following?
A. perform a pap smear
B. recommend that she restart estrogen replacement therapy
C. tell her that she can reduce her risk of dying of breast cancer by performing self-breast examinations monthly
D. order a bone density test to screen for osteoporosis
E. send a urine culture as a screening test for asymptomatic bacteruria
Correct Answer: D Section: (none)
Explanation: Explanations: Screening for osteoporosis in women 65 years old or older is a level B recommendation of the USPSTF, as detection and treatment of osteoporosis may reduce fracture risk. In women who have had a hysterectomy (with removal of the cervix) for reasons other than cervical cancer, pap smear screening of the vaginal cuff is not recommended and cytologic screening can be discontinued. Therapy with either estrogen alone (in women who do not have a uterus) or combined estrogen and progesterone (in women who have a uterus) in postmenopausal women is controversial. Based on findings of the Women's Health Initiative and other studies, the USPSTF gives a level D recommendation to the use of combined estrogen and progesterone therapy and level I recommendation for estrogen therapy alone for the prevention of chronic conditions. Screening for asymptomatic bacteruria in all populations other than pregnant women is given a level D recommendation. No benefit from the intervention has been found and overtreatment with antibiotics may produce harm. While mammography for breast cancer screening has been given a level B recommendation, both self-breast examination and clinical breast examination are level I recommendations, with insufficient evidence to show any benefit in morbidity or mortality.
According to the Centers for Disease Control, diseases of the heart make up the most common cause of death in women in this age group. Heart disease is responsible for approximately one-third of all deaths in women aged 65 and older. Malignant neoplasms make up the next largest cause of death, followed by cerebrovascular diseases and chronic lower respiratory diseases. PPV-23 is recommended for all adults over the age of 65 and at younger ages for individuals at high risk for pneumonia or complications of pneumonia. These include persons with diabetes mellitus, chronic obstructive pulmonary disease, coronary artery disease, and those who have had a splenectomy or are functionally asplenic. The PCV-7 is recommended for the routine vaccination of children. Hepatitis B vaccine is recommended universally for children and for adults who are at high risk for the disease based on profession or lifestyle. Hepatitis A vaccine is recommended for children who live in certain areas of the United States in which the disease is prevalent and may be offered electively to persons traveling to endemic areas. The MMR vaccine is recommended to all children but is not indicated in adults. Rubella vaccination is recommended for women of childbearing age who may become pregnant and who do not have immunity to rubella, in an effort to reduce the risk of congenital rubella infection
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.