A25-year-old African American female develops a large lesion on her ear lobe after having it pierced (see Figure). How would you advise this patient?
A. Surgical excision is curative.
B. This resulted from an infection that occurred when she had her ear pierced.
C. Recurrences of this problem are common.
D. She is likely to have reduced fertility.
E. Oral corticosteroids have been effective.
Correct Answer: C Section: (none)
Explanation:
Keloids occur at the site of injury, predominately in people with dark skin who have a genetic predisposition. The keloid is a form of benign tumor that consists of an overabundance of collagen that extends beyond the margins of the incision. Treatment options have only moderate success and include excision of the keloid with intralesional steroid injections. Recurrences of keloids, both at the original site and with subsequent injury/incision elsewhere in the body, are common. They are not associated with decreased fertility or other systemic processes
Question 502:
A 49-year-old male underwent his last chemotherapy session for testicular cancer 3 weeks ago and now is complaining of shortness of breath. Which of the following drugs is most probably causing his problems?
A. doxorubicin
B. etoposide
C. cisplatin
D. bleomycin
E. vincristine
Correct Answer: D Section: (none)
Explanation: Bleomycin is known to cause pulmonary fibrosis. Doxorubicin toxicity is predominantly manifested by leucopenia and cardiotoxicity. Etoposide is a podophyllotoxin derivative that inhibits topoisomerase which normally unwinds DNA and is associated with myelosuppression. Cisplatin is a platinum alkylating agent that can be nephrotoxic and ototoxic. Vincristine is a microtubule inhibitor that can result in peripheral neuropathy.
Question 503:
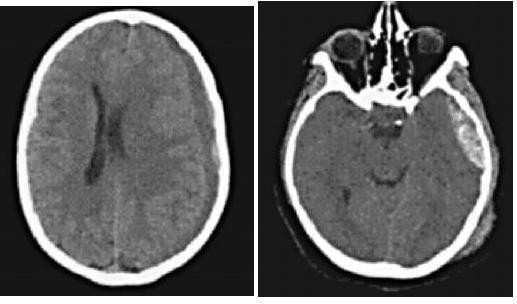
A 23-year old male driver involved in a head-on motor vehicle collision is brought to the ER. On initial evaluation in the trauma unit, his blood pressure is 180/70 and his pulse is 56. After initial evaluation and resuscitation you obtain a CT scan of his head
The finding on the imaging study is most commonly associated with injury to which of the following?
A. the bridging veins
B. the middle meningeal artery
C. the sagital sinus
D. the temporal artery
E. the epidural artery
Correct Answer: B Section: (none)
Explanation: The management of elevated intracranial pressure following traumatic injury has been extensively studied. Several interventions have been shown to be of benefit in the acute setting. The pressure can be relieved through mechanical means such as elevating the head of the bed to 30 degrees or by direct drainage of cerebrospinal fluid via a ventricular catheter. Administration of a hyperosmotic solution such as mannitol can decrease intracranial pressure by reducing brain water, increasing plasma volume and reducing blood viscosity. Additionally, if the ICP is refractory to these interventions, it is reasonable to consider a barbiturate coma or potentially a decompressive craniectomy. Hyperventilation is used only in the acute setting to keep PaCO2 around 35 mmHg, which functions to decrease intracranial pressure by decreasing intracranial blood volume through vasoconstriction. MRI would not be indicated initially, as it would not change your management. Severe head injuries are a frequent problem encountered in the field of trauma. CT scans are the primary diagnostic modality used to evaluate patients with suspected head injuries. Elevated intracranial pressure is a frequent result of severe brain injury either from brain swelling or mass effect from expanding hematomas. Subdural hemorrhages typically have a crescent shape and extend across suture lines covering the entire surface of one hemisphere. These are usually the result of the disruption of bridging veins. Epidural hematomas on the other hand have a biconvex lens appearance on CT scan. They typically develop afteran injury to the middle meningeal artery. Brain injury is generally greater in patients with subdural hematomas than in those with epidural hematomas.
Question 504:
A 23-year old male driver involved in a head-on motor vehicle collision is brought to the ER. On initial evaluation in the trauma unit, his blood pressure is 180/70 and his pulse is 56. After initial evaluation and resuscitation you obtain a CT scan of his head
The patient in the above scenario is then transported to the ICU. The most appropriate initial evaluation and management would include which of the following?
A. ensuring that his bed stays flat
B. aggressive hydration with a hypotonic solution
C. hyperventilation
D. needle drainage of the hematoma
E. MRI of the brain
Correct Answer: C Section: (none)
Explanation:
The management of elevated intracranial pressure following traumatic injury has been extensively studied. Several interventions have been shown to be of benefit in the acute setting. The pressure can be relieved through mechanical means such as elevating the head of the bed to 30 degrees or by direct drainage of cerebrospinal fluid via a ventricular catheter. Administration of a hyperosmotic solution such as mannitol can decrease intracranial pressure by reducing brain water, increasing plasma volume and reducing blood viscosity. Additionally, if the ICP is refractory to these interventions, it is reasonable to consider a barbiturate coma or potentially a decompressive craniectomy. Hyperventilation is used only in the acute setting to keep PaCO2 around 35 mmHg, which functions to decrease intracranial pressure by decreasing intracranial blood volume through vasoconstriction. MRI would not be indicated initially, as it would not change your management. Severe head injuries are a frequent problem encountered in the field of trauma. CT scans are the primary diagnostic modality used to evaluate patients with suspected head injuries. Elevated intracranial pressure is a frequent result of severe brain injury either from brain swelling or mass effect from expanding hematomas. Subdural hemorrhages typically have a crescent shape and extend across suture lines covering the entire surface of one hemisphere. These are usually the result of the disruption of bridging veins. Epidural hematomas on the other hand have a biconvex lens appearance on CT scan. They typically develop afteran injury to the middle meningeal artery. Brain injury is generally greater in patients with subdural hematomas than in those with epidural hematomas.
Question 505:
A 62-year-old man undergoes transplantation of a kidney from a cadaveric donor. The surgery is uncomplicated and his recovery proceeds well for the first week postoperatively. In the second postoperative week, he develops hypertension, peripheral edema, and decreased urinary output. He states that he has been taking his medications as ordered What is the most appropriate management at this time?
A. remove the donated kidney
B. pulse steroid dose and increase immunosuppresion
C. oral furosemide with follow-up in 1 week
D. hospitalization for IV furosemide, angiotensin-converting enzyme (ACE) inhibitor, and close monitoring
E. explain that the kidney transplant failed and that he needs to restart dialysis
Correct Answer: B Section: (none)
Explanation:
In transplant immunology, a wide variety of immune effector mechanisms are responsible for rejection. Acute rejection typically occurs in the first few days to weeks after organ transplantation.The primary mediator of this immune response is the T cell. Treatment of acute rejection usually involves pulse dose steroids and increased immunosuppression. Other forms of rejection include hyperacute rejection and chronic rejection. Hyperacute rejection is the result of preformed antibodies and occurs within hours of transplantation and leads to graft loss. Chronic rejection occurs on the scale of months to years after transplantation and is characterized by fibrosis and loss of normal histologic architecture
Question 506:
A 62-year-old man undergoes transplantation of a kidney from a cadaveric donor. The surgery is uncomplicated and his recovery proceeds well for the first week postoperatively. In the second postoperative week, he develops hypertension, peripheral edema, and decreased urinary output. He states that he has been taking his medications as ordered. What is the most likely cause of this condition?
A. hyperacute organ rejection
B. acute organ rejection
C. chronic organ rejection
D. congestive heart failure
E. failure of physician to restart him on his preoperative furosemide
Correct Answer: B Section: (none)
Explanation:
In transplant immunology, a wide variety of immune effector mechanisms are responsible for rejection. Acute rejection typically occurs in the first few days to weeks after organ transplantation.The primary mediator of this immune response is the T cell. Treatment of acute rejection usually involves pulse dose steroids and increased immunosuppression. Other forms of rejection include hyperacute rejection and chronic rejection. Hyperacute rejection is the result of preformed antibodies and occurs within hours of transplantation and leads to graft loss. Chronic rejection occurs on the scale of months to years after transplantation and is characterized by fibrosis and loss of normal histologic architecture.
Question 507:
A23-year-old male is brought by ambulance to the ER after being found in a house fire. He was in a closed room with a large amount of smoke and has sustained burns to his face, torso, arms, and legs. His pulse is 120, BP 110/55, and SpO2 92% on 2 L of oxygen by nasal cannula. Which of the following statements is true?
A. The burns should be covered in cool, moist dressings.
B. An inhalation injury is unlikely since he is able to oxygenate on minimal supplementation.
C. Fluids should be limited to prevent pulmonary edema after his smoke inhalation.
D. This patient meets criteria for transfer to a dedicated burn center.
E. Depth of the burn does not affect the management.
Correct Answer: D Section: (none)
Explanation:
Like other trauma patients, the initial management of burn patients is crucial in improving survival and function. Inhalation injury should be suspected in anyone with a history of confinement in smoke, facial burns, singed eyebrows or nasal hairs, carbonaceous sputum, or carboxyhemoglobin levels greater than 10%. These patients sometimes look stable initially but soon develop airway edema. These patients should be placed on high-flow oxygen and observed closely. There should be a very low threshold for endotracheal intubation to protect the airway. Burn patients require large volume fluid resuscitation that should begin immediately. If patients develop pulmonary edema, they should be intubated. Fluid resuscitation should not be withheld to prevent intubation. Heat loss is also a major concern in burn patients who have lost their thermoprotective skin covering. They should be wrapped in warm, moist dressings. Depth of burn affects management in resuscitation efforts, as well as need for debridement or escharotomy, and should be evaluated in every patient. The American Burn Association recommends transfer to a burn center for patients with: · Partial thickness and full thickness burns of >10% of total body surface area TBSA in patients with age <10 years old or >50 years old · Partial or full thickness burns of >20% in patients of any other age · Partial or full thickness burns involving face, hands, feet, genitalia, or perineum · Full thickness burns of >5% TBSA in any age group · Significant electrical or chemical burns · Inhalation injury
Question 508:
An 18-year-old male is brought to the ED after sustaining a stab wound to the left chest that is medial and superior to the nipple. He was unresponsive at the scene and intubated by the emergency medical technician (EMT) team. His pulse is 140 and BP is 60/30 after receiving 1 L of lactated Ringers solution and 2 units of blood during his transport. On auscultation there are no breath sounds on the left. His trachea is midline. He has no evidence of neck vein distention.
Which of the following statements is true?
A. Cardiac tamponade is unlikely since there is no evidence of neck vein distention.
B. A left chest tube should be placed immediately.
C. Given the probability of a cardiac injury, an emergent thoracotomy should be performed in the ED.
D. An aortic angiogram should be ordered immediately to assess for aortic injury.
E. No intervention should be performed until a chest x-ray is completed to provide more information.
Correct Answer: B Section: (none)
Explanation:
One of every four trauma deaths in North America is due to thoracic trauma. Many deaths from thoracic trauma can be prevented with prompt diagnosis and treatment of injuries. The first step in the evaluation of any trauma patient is the primary survey, or ABCDE (airway, breathing, circulation, disability, exposure). First you would evaluate the airway. In this case, an endotracheal tube was placed at the scene. It would be important to evaluate this airway's adequacy of placement using a capnometer to assess end-tidal CO2 and auscultation of the breath sounds. Next you would assess breathing. Auscultation in this patient reveals an absence of breath sounds on the left. This must be resolved before moving on to circulation. This could be the result of placing the endotracheal tube in too far into the right mainstem, which is easily checked by withdrawing the endotracheal tube 2 cm.
The other possibilities are life-threatening emergencies, including a tension pneumothorax or a hemothorax. Given the fact that the patient is unstable and there is a history of penetrating chest trauma, a chest tube should be placed immediately without the delay of a chest x-ray. A tube thoracostomy in this patient will be diagnostic and also therapeutic. Ahypovolemic patient with cardiac tamponade may not have neck vein distension. ED thoracotomies should only be performed in a pulseless patient. All other patients requiring thoracotomy should go to the OR. This patient is unstable and as such should not be taken to angiogram.
Question 509:
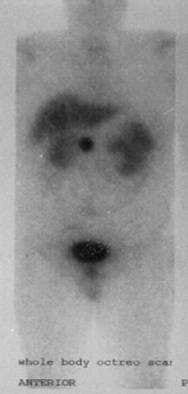
A40-year-old man presents with chronic diarrhea and peptic ulcer disease refractory to medical management with proton pump inhibitors. An octreotide scan is shown in Figure which corresponds to an area near the head of the pancreas. Which of the following factors directly results in the release of the hormone produced by this tumor?
A. secretin
B. glucagon
C. antral pH <2.0
D. vagus nerve
E. somatostatin
Correct Answer: D Section: (none)
Explanation:
This patient has a gastrinoma, seen in Zollinger-Ellison syndrome, and should also be evaluated for possible MEN I. Gastrin is a GI hormone that is released from the antral G cells of the stomach to regulate acid secretion by the gastric parietal cells. It is released when the stomach gets the signal that is needed to initiate the digestion process, and also acts to stimulate chief cells to secrete pepsinogen and to increase gastric mucosal blood flow. Known stimulants for the release of gastrin include: vagal stimulation, calcium, alcohols in the stomach, proteins/amino acids in the stomach, antral distention, and gastric pH greater than
3. Antral pH less than 2 inhibits gastrin release, as does somatostatin. Secretin has no effect or decreases gastrin levels in healthy patients, but it increases gastrin release in patients with Zollinger-Ellison syndrome. Glucagon has little or no effect on gastrin release.
Question 510:
A 72-year-old woman undergoes a sigmoid colectomy for diverticulitis. Postoperatively, she develops a wound infection for which she is transferred to the ICU for 2 days because of hypotension. Which of the following would have had the most effect on reducing her risk of developing complications?
A. preoperative treatment of her concomitant urinary tract infection
B. nurses changing gloves in between their patient assessments so they don't have to wash their hands as often
C. using a preoperative antibiotic specific for E. coli, the most common intestinal flora
D. giving preoperative antibiotics immediatel after the skin incision
E. treatment of the infected wound with an antibiotic only
Correct Answer: A Section: (none)
Explanation: Wound infection is a complication of surgery that can lead to a great deal of morbidity and longer hospital stay. Prevention of wound infection includes perioperative antibiotics, which should be at their peak tissue concentration at the time of skin incision. This means they should be given at least 30 minutes prior to incision. Patients who have other infections, such as urinary tract infections, are at increased risk for wound infection. Bowel surgery exposes the wound to the normal intestinal flora, the most common being Bacteroides. Washing hands is an essential part of preventing spread of infectious pathogens between patients. Using gloves is not a substitute for good hand hygiene. Once a wound is infected, it must be opened and drained. Antibiotic therapy alone is not adequate.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.