A55-year-old man with hepatic cirrhosis from alcohol abuse presents with a massive hematemesis. This is his third admission for upper GI hemorrhage in the past 2 months. He is currently receiving appropriate therapy for liver failure, including a beta-blocker and diuretics. He is lethargic and confused. His pulse is 100 and blood pressure is 85/40. His initial hematocrit is 20.
Endoscopic attempts to control the bleeding are initially successful, but the patient has a recurrent bleed 2 days later. The medicine team obtains a surgical consultation for placement of a shunt.Which of the following statements is true?
A. The best shunts are nonselective, meaning that they divert all blood from the portal system.
B. Synthetic graft materials should never be used because of the risk of infection.
C. A mesocaval shunt involves connecting the superior mesenteric vein (SMV) to the inferior vena cava (IVC).
D. Encephalopathy rarely worsens after the placement of the shunt. In fact, it often improves in these patients.
E. Postoperative mortality for emergency shunts is related more to the type of shunt placed rather than the degree of hepatic failure in the patient.
Correct Answer: C Section: (none)
Explanation:
In patients with liver failure, the source of an upper GI bleed is esophageal varices in 50%, gastritis in 30%, and duodenal ulcers in only about 10%. Esophageal variceal bleeding is a potentially fatal complication of portal hypertension. The initial management should include fluid resuscitation and replacement of blood and clotting factors as needed. The second step is to control the source of bleeding. Medical management may include vasopressin or octreotide. Once the patient is stabilized, endoscopic evaluation of the bleeding is crucial. It can be both diagnostic and therapeutic. Endoscopic techniques for controlling hemorrhage can include sclerotherapy, banding, or balloon tamponade. If these methods are ineffective, or the patient has numerous recurrences, portal shunts can be considered. TIPS have increased in popularity as a method for portal decompression. This can be performed in the acute setting. Surgical shunts are also an option, but are primarily reserved for stable patients with recurrent bleeding episodes and not performed in an acutely unstable patient. Mesocaval shunts connect the SMV to the IVC in a variety of manners. Splenorenal shunts are actually the most common type of shunt. Nonselective shunts that completely divert portal blood flow from the liver can actually increase hepatic encephalopathy. Most surgeons prefer selective shunts, which preserve a component of hepatic blood flow and thus function. Synthetic graft material can be safely used to create the shunts. Postoperative mortality is directly related to the patient's preprocedure medical condition and degree of hepatic failure.
Question 582:
A55-year-old man with hepatic cirrhosis from alcohol abuse presents with a massive hematemesis. This is his third admission for upper GI hemorrhage in the past 2 months. He is currently receiving appropriate therapy for liver failure, including a beta-blocker and diuretics. He is lethargic and confused. His pulse is 100 and blood pressure is 85/40. His initial hematocrit is 20. After fluid resuscitation, which of the following is the most appropriate management strategy?
A. The transplant team should be called immediately.
B. The bleeding is probably secondary to an uncontrolled duodenal ulcer related to his alcohol use.
C. Red blood cells should be administered immediately, but fresh frozen plasma should be withheld if possible.
D. Endoscopic control options include sclerotherapy and banding.
E. Transjugular intrahepatic portal systemic shunt (TIPS) is not an option in the immediate period.
Correct Answer: D Section: (none)
Explanation:
In patients with liver failure, the source of an upper GI bleed is esophageal varices in 50%, gastritis in 30%, and duodenal ulcers in only about 10%. Esophageal variceal bleeding is a potentially fatal complication of portal hypertension. The initial management should include fluid resuscitation and replacement of blood and clotting factors as needed. The second step is to control the source of bleeding. Medical management may include vasopressin or octreotide. Once the patient is stabilized, endoscopic evaluation of the bleeding is crucial. It can be both diagnostic and therapeutic. Endoscopic techniques for controlling hemorrhage can include sclerotherapy, banding, or balloon tamponade. If these methods are ineffective, or the patient has numerous recurrences, portal shunts can be considered. TIPS have increased in popularity as a method for portal decompression. This can be performed in the acute setting. Surgical shunts are also an option, but are primarily reserved for stable patients with recurrent bleeding episodes and not performed in an acutely unstable patient. Mesocaval shunts connect the SMV to the IVC in a variety of manners. Splenorenal shunts are actually the most common type of shunt. Nonselective shunts that completely divert portal blood flow from the liver can actually increase hepatic encephalopathy. Most surgeons prefer selective shunts, which preserve a component of hepatic blood flow and thus function. Synthetic graft material can be safely used to create the shunts. Postoperative mortality is directly related to the patient's preprocedure medical condition and degree of hepatic failure.
Question 583:
Which of the following statements is true concerning Meckel's diverticulum?
A. It is found within 2 in. of the ileocecal valve.
B. It represents a remnant of the embryonic vitelline duct.
C. Ectopic colonic epithelium is found in it.
D. Diagnosis is best made by CT scan.
E. The diverticulum is usually found on the mesenteric border of the bowel.
Correct Answer: B Section: (none)
Explanation:
Meckel's diverticuli are usually found incidentally, although they can present with painless lower GI bleeding or inflammation (often confused with acute appendicitis). They are usually found within 2 ft of the ileocecal valve.They represent a remnant of the vitelline (or omphalomesenteric) duct and are found on the antimesenteric side of the ileum. They often contain ectopic gastric mucosa. Acid secretion from this leads to ileal ulceration and bleeding. They can be diagnosed using nuclear medicine scans (technetium pertechnetate) and the treatment is surgical resection.
Question 584:
A1-month-old female presents after an episode of bilious emesis. She became irritable 12 hours ago, began vomiting 6 hours ago, and is now lethargic. She had one small stool that was somewhat bloody 2 hours ago.
Which of the following statements is true?
A. An upper GI contrast study should be obtained immediately.
B. The most likely explanation is pyloric stenosis.
C. The patient should be admitted for IV fluid resuscitation and observation. If she does not improve over the next 24 hours, a surgical consultation should be obtained.
D. An air contrast enema is the most appropriate next step.
E. A nasogastric tube should be inserted and IV antibiotics started to treat probable necrotizing enterocolitis.
Correct Answer: A Section: (none)
Explanation:
Any infant or child that presents with bilious emesis should be evaluated immediately for malrotation with midgut volvulus. This is a surgical emergency since the volvulus can compromise the vascular supply to the intestine. Malrotation is a congenital disorder wherein the normal prenatal rotation of the midgut is incomplete and results in the cecum remaining in the epigastrium with a narrow superior mesenteric artery (SMA) pedicle. When this happens, bands form between the cecum and the abdominal wall ("Ladd's bands"). Avolvulus may result around the shortened mesentery, cutting off the vascular supply to the midgut and causing obstruction. In volvulus, patients present with acute onset of bilious emesis and later with bloody stools or hemodynamic instability. The diagnosis of malrotation can be best made with an upper GI contrast study, which will show the duodenojejunal junction displaced to the right of midline. Sometimes this can also reveal volvulus. Patients with volvulus must be taken emergently to the OR to reduce the volvulus. If intestinal ischemia is advanced, a significant portion of small bowel may have to be removed, resulting in "short gut syndrome." In this patient presenting with bilious emesis, malrotation with volvulus must be considered and addressed early. The correct answer is to get an upper GI contrast study to evaluate for malrotation and obtain a surgical consultation. Observation (choice C) may result in intestinal ischemia or death. Pyloric stenosis (choice B) presents with nonbilious emesis. Choice D refers to intussusception, which often presents with bloody stools but bilious emesis is unlikely. Necrotizing enterocolitis (choice E) can also present with bloody stools, but usually occurs in premature infants as they approach full enteral feeds.
Question 585:
A 4-week-old, previously healthy male presents with projectile emesis after feeds. His mother states that he has had 2 weeks of postprandial emesis, which became projectile in the past 2 days. She states that it looks like formula and has never been bilious.
Which of the following statements is true?
A. Physical examination is almost always normal in patients with this condition.
B. Upper gastrointestinal (GI) contrast study is the best diagnostic option.
C. This patient should be taken emergently to the operating room (OR) once the diagnosis is made.
D. If uncorrected, these infants will progress to complete obstruction.
E. Surgical therapy involves bypassing the site of obstruction.
Correct Answer: D Section: (none)
Explanation:
Pyloric stenosis usually presents in the first 48 weeks of life. Parents usually report nonbilious emesis after feeding, which progresses to a projectile nature. Untreated, this will become a complete obstruction. On examination, an "olive sign" or mass in the right upper quadrant is often found. Ultrasound is the best radiologic test. These infants may present with dehydration and metabolic abnormalities from the emesis. The most common abnormality is hypokalemic, hypochloremic metabolic alkalosis. While surgical correction is urgent, it is not emergent. These infants should be resuscitated with IV fluids and their metabolic derangements corrected before an operation. The surgical treatment is a pyloromyotomy, which involves splitting the hypertrophic muscles of the pylorus while keeping the mucosa intact. This can be performed either open or laparoscopically. Patients are usually allowedto feed within hours of their operation.
Question 586:
A 10-month-old male presents with a 12-hour history of episodes of crying, holding his stomach, and
bending over in pain. The parents report one "reddish" stool. He has no past medical history or episodes of
similar events. He did have 24 hours of viral symptoms, which resolved a few days ago.
The following study was obtained.
Which of the following statements is true?
A. The initial treatment for this child involves emergent laparotomy.
B. Air contrast enema can be diagnostic AND therapeutic.
C. Colonic mass is the usual source of this problem in a child.
D. "Dance's sign" is the appearance on xray of "telescoped" intestine.
E. Recurrence is likely after treatment.
Correct Answer: B Section: (none)
Explanation:
Intussusception is usually seen in children 812 months of age. They present with paroxysmal, crampy abdominal pain, and sometimes emesis. "Currant-jelly" stools are sometimes seen. They usually report a history of GI viral infection in the recent past. Enlarged Peyer's patches are usually the lead point of the intussusception. Polyps, tumors, and Meckel's diverticulum are less frequent causes. On examination, these children may have a mass in the epigastrium or right upper quadrant with an absence of intestine in the right lower quadrant. This is referred to as "Dance's sign." The diagnostic tool of choice is air contrast enema. This is also therapeutic in 6090% of cases. If the intussusception cannot be reduced by the enema, laparotomy is required to prevent bowel ischemia. Compromised bowel is resected at that time. Only 5% of children have a recurrence after successful reduction.
Question 587:
1. A22-year-old male presents to the emergency department (ED) with complaints of right-sided chest pain and dyspnea. He has no other significant medical history. There is no history of trauma. On examination, he has a pulse of 95, BP of 110/70, and SpO2 of 95% on 2 L. A chest x-ray reveals a large right pneumothorax.
Which of the following statements is true?
A. Since the patient is hemodynamically stable, he can be observed with oxygen supplementation, pain control, and serial chest x-rays.
B. The patient is likely to have a tall, thin habitus.
C. This condition is probably due to small lacerations in the apex of the right lung.
D. His risk of recurrence is 10%.
E. Recurrences are usually on the contralateral side since adhesions prevent recurrence on the ipsilateral side.
Correct Answer: B Section: (none)
Explanation:
Spontaneous pneumothorax is usually found in young males. A tall, thin habitus is common. Eighty-five percent of patients are found to have pulmonary blebs on the affected side. The correct management is placement of a chest tube, pain control, oxygen supplementation, and serial chest x-rays to monitor resolution. Thoracotomy is required if the pneumothorax does not resolve with a chest tube or if there is a persistent air leak. Bleb resection and pleurodesis is usually performed at the time of operation to prevent future bleb rupture and to promote adhesion of the lung to the chest wall. Thoracotomy is also offered to patients after a recurrence to prevent future episodes. Fifty percent of patients will have a recurrence on the ipsilateral side after a spontaneous pneumothorax.
Question 588:
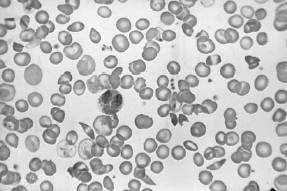
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101°F. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure
.
The patient develops pain in both hips and an MRI shows avascular necrosis. This is likely due to which of the following?
A. osteomyelitis due to Salmonella infection
B. HIV infection
C. a pituitary tumor causing Cushing syndrome
D. associated arthritis
E. chronic ischemia to the head of the femur
Correct Answer: E Section: (none)
Explanation:
This patient has sickle cell anemia. This is evident from sickle cells forms on the peripheral blood smear in
Figure 1-13. Pain medication is an important initial concern. It is often difficult to determine whether a patient in sickle cell crisis has an ongoing infection. Infections can precipitate sickle cell crisis. With respect to community-acquired pneumonia, the diagnosis is difficult. A patient with sickle cell crisis can have fever as a result of the sickle crisis. They can have an increased respiratory rate, physical examination, and CXR findings which suggest pneumonia as a result of pulmonary infarctions. A white blood count can be elevated due to marrow stimulation. In the presence of the acute chest syndrome, characterized by chest pain, hypoxia, and CXR infiltrates, antibiotics would be indicated. Without further information, it is hard to decide to empirically start broad-spectrum antibiotics for community-acquired pneumonia. Transfusions should generally be avoided in patients with sickle cell anemia who are not symptomatic due to the anemia. Since patients in sickle cell crisis have intravascular hemolysis, their reticulocyte counts are usually high and they can replace their blood quickly. Repeated small transfusions will lead to autoantibodies that will make further transfusions difficult. Arterial blood gas determination should not be the first step, given the above information. A CT scan of the abdomen is not indicated given the nonspecific nature of the patient's abdominal findings. Parvovirus B19 can cause aplastic crisis in patients with hemoglobinopathies, including sickle cell disease. A tip to this diagnosis is the decreased reticulocyte count in a patient who normally would have a high reticulocyte count. Given the information listed above, there is no indication for broad-spectrum antibiotics. Splenectomy is not a reasonable alternative at this point. Patients with sickle cell disease have autosplenectomy by the time they are adults. A bone marrow biopsy maybe indicated because of the low platelet count, but not initially. GnCSF is not indicated because the patient does not have neutropenia. Patients with sickle cell disease typically have isosthenuria.
This is due to repeated infarction of the renal papilli. This causes destruction and interference with the counter current mechanism that causes urine concentration. As a result, patients with sickle cell anemia have the inability to concentrate their urine. This results in fluid and electrolyte abnormalities. Patients in sickle cell crisis are usually fluid depleted. This and the sickled blood cells cause hyperviscosity and microinfarctions. There is no evidence that the patient has diabetes insipidus, which usually has a urine specific gravity less than 1.005. Patients with UTIs do not have isosthenuria due to RBCs and WBCs that increase the urine specific gravity. Sickle cell patients may have zinc deficiency, but this is not a cause of isosthenuria.
Question 589:
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101°F. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure .
Oxygen and IV fluids are given. A urine specific gravity is 1.010. Which of the following is the best explanation for this?
A. The patient is volume overloaded and fluid should be stopped.
B. The patient has developed diabetes insipidus.
C. The patient has developed a UTI leading to frequent urination.
D. This finding is secondary to repeated infarction of the renal papillae.
E. This complication is due to zinc wasting.
Correct Answer: D Section: (none)
Explanation:
This patient has sickle cell anemia. This is evident from sickle cells forms on the peripheral blood smear in Figure 1-13. Pain medication is an important initial concern. It is often difficult to determine whether a patient in sickle cell crisis has an ongoing infection. Infections can precipitate sickle cell crisis. With respect to community-acquired pneumonia, the diagnosis is difficult. A patient with sickle cell crisis can have fever as a result of the sickle crisis. They can have an increased respiratory rate, physical examination, and CXR findings which suggest pneumonia as a result of pulmonary infarctions. A white blood count can be elevated due to marrow stimulation. In the presence of the acute chest syndrome, characterized by chest pain, hypoxia, and CXR infiltrates, antibiotics would be indicated. Without further information, it is hard to decide to empirically start broad-spectrum antibiotics for community-acquired pneumonia. Transfusions should generally be avoided in patients with sickle cell anemia who are not symptomatic due to the anemia.
Since patients in sickle cell crisis have intravascular hemolysis, their reticulocyte counts are usually high and they can replace their blood quickly. Repeated small transfusions will lead to autoantibodies that will make further transfusions difficult. Arterial blood gas determination should not be the first step, given the above information. A CT scan of the abdomen is not indicated given the nonspecific nature of the patient's abdominal findings. Parvovirus B19 can cause aplastic crisis in patients with hemoglobinopathies, including sickle cell disease. A tip to this diagnosis is the decreased reticulocyte count in a patient who normally would have a high reticulocyte count. Given the information listed above, there is no indication for broad-spectrum antibiotics. Splenectomy is not a reasonable alternative at this point. Patients with sickle cell disease have autosplenectomy by the time they are adults. A bone marrow biopsy maybe indicated because of the low platelet count, but not initially. GnCSF is not indicated because the patient does not have neutropenia. Patients with sickle cell disease typically have isosthenuria.
This is due to repeated infarction of the renal papilli. This causes destruction and interference with the counter current mechanism that causes urine concentration. As a result, patients with sickle cell anemia have the inability to concentrate their urine. This results in fluid and electrolyte abnormalities. Patients in sickle cell crisis are usually fluid depleted. This and the sickled blood cells cause hyperviscosity and microinfarctions. There is no evidence that the patient has diabetes insipidus, which usually has a urine specific gravity less than 1.005. Patients with UTIs do not have isosthenuria due to RBCs and WBCs that increase the urine specific gravity. Sickle cell patients may have zinc deficiency, but this is not a cause of isosthenuria.
Question 590:
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101°F. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure
.
A CBC with differential and platelets later shows the Hgb to be 6.4, white blood count is 2100 with 85% polymorphonuclear forms, platelet count is 100, and the reticulocyte countis 0.5. Which of the following would be an appropriate next test?
A. serum antibody to parvovirus B19
B. broad-spectrum antibiotics for sepsis
C. consideration for splenectomy
D. a bone marrow biopsy
E. administration of granulocyte colonystimulating factor (GnCSF)
Correct Answer: A Section: (none)
Explanation:
This patient has sickle cell anemia. This is evident from sickle cells forms on the peripheral blood smear in Figure 1-13. Pain medication is an important initial concern. It is often difficult to determine whether a patient in sickle cell crisis has an ongoing infection. Infections can precipitate sickle cell crisis. With respect to community-acquired pneumonia, the diagnosis is difficult. A patient with sickle cell crisis can have fever as a result of the sickle crisis. They can have an increased respiratory rate, physical examination, and CXR findings which suggest pneumonia as a result of pulmonary infarctions. A white blood count can be elevated due to marrow stimulation. In the presence of the acute chest syndrome, characterized by chest pain, hypoxia, and CXR infiltrates, antibiotics would be indicated. Without further information, it is hard to decide to empirically start broad-spectrum antibiotics for community-acquired pneumonia. Transfusions should generally be avoided in patients with sickle cell anemia who are not symptomatic due to the anemia. Since patients in sickle cell crisis have intravascular hemolysis, their reticulocyte counts are usually high and they can replace their blood quickly. Repeated small transfusions will lead to autoantibodies that will make further transfusions difficult. Arterial blood gas determination should not be the first step, given the above information. A CT scan of the abdomen is not indicated given the nonspecific nature of the patient's abdominal findings. Parvovirus B19 can cause aplastic crisis in patients with hemoglobinopathies, including sickle cell disease. A tip to this diagnosis is the decreased reticulocyte count in a patient who normally would have a high reticulocyte count. Given the information listed above, there is no indication for broad-spectrum antibiotics. Splenectomy is not a reasonable alternative at this point. Patients with sickle cell
disease have autosplenectomy by the time they are adults. A bone marrow biopsy maybe indicated
because of the low platelet count, but not initially. GnCSF is not indicated because the patient does not
have neutropenia.
Patients with sickle cell disease typically have isosthenuria.
This is due to repeated infarction of the renal papilli. This causes destruction and interference with the
counter current mechanism that causes urine concentration. As a result, patients with sickle cell anemia
have the inability to concentrate their urine. This results in fluid and electrolyte abnormalities. Patients in
sickle cell crisis are usually fluid depleted. This and the sickled blood cells cause hyperviscosity and
microinfarctions. There is no evidence that the patient has diabetes insipidus, which usually has a urine
specific gravity less than 1.005. Patients with UTIs do not have isosthenuria due to RBCs and WBCs that
increase the urine specific gravity. Sickle cell patients may have zinc deficiency, but this is not a cause of
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.