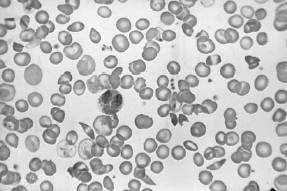
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101°F. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure
.
Among the initial orders for this patient should be which of the following?
A. broad-spectrum antibiotics for community-acquired pneumonia
B. type and hold for 2 units packed RBCs
C. an arterial blood gas
D. a CT scan of the abdomen
E. analgesics
Correct Answer: E Section: (none)
Explanation:
This patient has sickle cell anemia. This is evident from sickle cells forms on the peripheral blood smear in Figure 1-13. Pain medication is an important initial concern. It is often difficult to determine whether a patient in sickle cell crisis has an ongoing infection. Infections can precipitate sickle cell crisis. With respect to community-acquired pneumonia, the diagnosis is difficult. A patient with sickle cell crisis can have fever as a result of the sickle crisis. They can have an increased respiratory rate, physical examination, and CXR findings which suggest pneumonia as a result of pulmonary infarctions. A white blood count can be elevated due to marrow stimulation. In the presence of the acute chest syndrome, characterized by chest pain, hypoxia, and CXR infiltrates, antibiotics would be indicated. Without further information, it is hard to decide to empirically start broad-spectrum antibiotics for community-acquired pneumonia. Transfusions should generally be avoided in patients with sickle cell anemia who are not symptomatic due to the anemia. Since patients in sickle cell crisis have intravascular hemolysis, their reticulocyte counts are usually high and they can replace their blood quickly. Repeated small transfusions will lead to autoantibodies that will make further transfusions difficult. Arterial blood gas determination should not be the first step, given the above information. A CT scan of the abdomen is not indicated given the nonspecific nature of the patient's abdominal findings. Parvovirus B19 can cause aplastic crisis in patients with hemoglobinopathies, including sickle cell disease. A tip to this diagnosis is the decreased reticulocyte count in a patient who normally would have a high reticulocyte count. Given the information listed above, there is no indication for broad-spectrum antibiotics. Splenectomy is not a reasonable alternative at this point. Patients with sickle cell disease have autosplenectomy by the time they are adults. A bone marrow biopsy maybe indicated because of the low platelet count, but not initially. GnCSF is not indicated because the patient does not have neutropenia. Patients with sickle cell disease typically have isosthenuria.
This is due to repeated infarction of the renal papilli. This causes destruction and interference with the counter current mechanism that causes urine concentration. As a result, patients with sickle cell anemia have the inability to concentrate their urine. This results in fluid and electrolyte abnormalities. Patients in sickle cell crisis are usually fluid depleted. This and the sickled blood cells cause hyperviscosity and microinfarctions. There is no evidence that the patient has diabetes insipidus, which usually has a urine specific gravity less than 1.005. Patients with UTIs do not have isosthenuria due to RBCs and WBCs that increase the urine specific gravity. Sickle cell patients may have zinc deficiency, but this is not a cause of isosthenuria.
Question 592:
A 74-year-old female with a history of hypertension and hypothyroidism is admitted with easy bruising, guaiac positive stools, and anemia (Hgb 8.1 g/dL). Screening coagulation tests reveal a prolonged activated partial thromboplastin time (aPTT) with a normal prothrombin time (PT) and platelet count.
What is the next step in the diagnosis of this woman's problem?
A. Perform upper and lower endoscopy with biopsies.
B. Check factors II, VII, IX, and X levels.
C. Check factor VII level.
D. Check factors XI, VII, IX, and VIII levels
E. Check an aPTT 1:1 mix with normal plasma and 1-hour incubation.
Correct Answer: E Section: (none)
Explanation:
A 1:1 mixing study is done when the PT or PTT is prolonged. The patient's plasma is mixed with normal plasma and the abnormal test is repeated. If the mixing of normal plasma corrects the abnormal test (PT or PTT), then a factor deficiency is suggested; otherwise, an inhibitor is suspected. Similarly, an incubated mixing study is done 1 hour (and occasionally 2 hours) after mixing of the patient plasma with normal plasma. It is used to differentiate a lupus anticoagulant from factor inhibitors.
Question 593:
A 32-year-old male is seen in the ER with a nondisplaced fracture of the ulna after a fall. Incidentally, the intern noticed that the patient is jaundiced and has a palpable spleen. He orders a CBC which shows a Hgb of 10.2 g/dL. The patient reveals that he has chronic anemia and intermittently has been prescribed iron. On further questioning, he says that he had a cholecystectomy at age 23 and that he has family members with similar symptoms. The intern reviews the peripheral smear and finds spherocytes. What would be the best way to confirm this man's diagnosis?
A. splenectomy
B. Hgb electrophoresis
C. osmotic fragility
D. G6PD level
E. indirect Coombs test
Correct Answer: C Section: (none)
Explanation:
Hereditary spherocytosis (HS) is a familial hemolytic disorder with clinical features, ranging from an asymptomatic condition to a fulminant hemolytic anemia. The morphologic hallmark of HS is the microspherocyte, which result from membrane protein defects leading to cytoskeleton instability. Spectrin deficiency leads to loss of erythrocyte surface area, which produces spherical RBCs. Spherocytic RBCs are culled from the circulation by the spleen leading to the development of splenomegaly. Spectrin deficiency and the degree of deficiency correlate with the extent of spherocytosis, the degree of abnormality on osmotic fragility test results, and the severity of hemolysis. Hemolysis primarily is confined to the spleen and, therefore, is extravascular.
Although four abnormalities in red cell membrane proteins have been identified, spectrin deficiency is the most common. Spectrin deficiency results from impaired synthesis, whereas in other instances, it is caused by quantitative or qualitative deficiencies of other proteins that integrate spectrin into the cell membrane. In the absence of these binding proteins, free spectrin is degraded, leading to spectrin deficiency. The major complications are aplastic or megaloblastic crisis, hemolytic crisis, cholecystitis and cholelithiasis, and severe neonatal hemolysis. The classic laboratory features of HS include minimal or no anemia, reticulocytosis, an increased mean corpuscular hemoglobin concentration (MCHC), spherocytes on the peripheral blood smear, hyperbilirubinemia, and abnormal results on the osmotic fragility test. The most sensitive test to help detect HS is the osmotic fragility test performed after incubating RBCs for 1824 hours under sterile conditions at 37°C. Osmoti c fragility measures RBC resistance to hemolysis when exposed to a series of increasingly dilute saline solutions. The sooner hemolysis occurs, the greater the osmotic fragility of the cells.
Question 594:
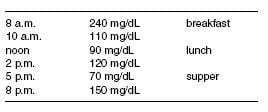
An 18-year-old man with a history of type I diabetes since age 14 presents to the clinic for further management. He notes several episodes of hypoglycemia at around 2 a.m. that awaken him from sleep since starting on his school's tennis team. He practices in the afternoon. His 8 a.m. glucose readings prior to breakfast are all greater than 200 mg/dL. His current insulin regimen is as follows: Breakfast: NPH 20 units with 5 units of regular insulin Supper: NPH 15 units with 5 units of regular insulin His average fingerstick glucose readings over the past week are as follows:
Which of the following recommendations would most likely improve his glucose control?
A. Discontinue insulin and start metformin.
B. Schedule NPH at bedtime instead of before supper.
C. Discontinue regular insulin at supper.
D. Advise the coach that he cannot play tennis.
E. Increase the regular insulin at breakfast.
Correct Answer: B Section: (none)
Explanation:
The patient has type I diabetes, therefore oral agents are contraindicated. The glucose pattern he has is known as the Somogyi phenomenon. His increased activity has made him more insulin sensitive, especially at the time of the day that he is most at risk of hypoglycemic reactions. When NPH is given at supper time, the peak action will be ~2 a.m. Changing the timing of the NPH to bedtime, will advance the peak to ~46 a.m., a time when the patient is becoming increasingly insulin resistant (Dawn phenomenon). As his glucose is already increasing at supper, discontinuing the regular insulin at that time may avoid nocturnal hypoglycemia, but at the expense of higher glucose values. Increasing the regular insulin at breakfast will likely cause hypoglycemia prior to lunch.
Question 595:
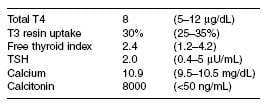
A28-year-old woman was noted to have a 3 cm thyroid nodule at the time of a well-woman examination. Her mother and maternal aunt died of thyroid cancer. On examination, her BP was 160/105, heart rate 90/ minute. Laboratory studies:
Which of the following is the most likely diagnosis?
A. papillary thyroid cancer
B. follicular carcinoma with T3 toxicosis
C. medullary thyroid carcinoma
D. hyperfunctioning thyroid adenoma
E. Hashimoto thyroiditis
Correct Answer: C Section: (none)
Explanation:
The patient has a strong family history of thyroid cancer and has a thyroid nodule, hypertension, tachycardia, and hypercalcemia. These are hallmarks of Multiple Endocrine Neoplasia Type 2 (MEN2) syndrome, which is associated with medullary thyroid cancer, pheochromocytoma, and hyperparathyroidism. The very high calcitonin level is an excellent tumor marker for medullary thyroid cancer and a fine needle aspiration is not indicated. She will need to have an evaluation and treatment for pheochromocytoma prior to treatment of her thyroid cancer.
Question 596:
A40-year-old woman presents with headaches and visual disturbances for the past 6 months. She suddenly developed amenorrhea 2 years ago. One year ago, she noticed milky discharge from her left breast. The most likely diagnosis is which of the following?
A. prolactinoma
B. premature ovarian failure
C. Kallman syndrome
D. Sheehan syndrome
E. polycystic ovarian syndrome (PCOS)
Correct Answer: A Section: (none)
Explanation: Galactorrhea with amenorrhea is consistent with hyperprolactinemia. The additional history of headache and possible visual field changes or cranial nerve abnormalities is strongly suggestive of a pituitary tumor. In this setting, the most likely diagnosis is prolactinoma. Ovarian failure, Kallman syndrome, and Sheehan syndrome would not present with galactorrhea. Kallman syndrome is associated with primary amenorrhea and anosmia. PCOS presents with a long history of irregular cycles and hyperandrogenism
Question 597:
A 25-year-old man presents to the ER with a 3-month history of intermittent pounding headaches, sweating, and palpitations. He denies any symptoms of depression or anxiety. On examination, he is a thin gentleman, BP 240/120, heart rate 110/minute, thyroid not enlarged. There is no prior history of hypertension.
The most likely diagnosis is which of the following?
A. carcinoid syndrome
B. thyroid cancer
C. pheochromocytoma
D. aldosteronoma E. renal artery stenosis
Correct Answer: C Section: (none)
Explanation:
The classic triad of pheochromocytoma is sweating, headache, and palpitations. When these are associated with hypertension, they have a sensitivity and specificity of >90% for the diagnosis. Paroxysms are not a component of aldosterone secreting tumors or renal artery stenosis. Hyperthyroidism and panic attacks would be in the differential diagnosis, but thyroid cancer is not associated with hypertension.
Question 598:
A 24-year-old male presents to the office for evaluation of a nodule on his left testicle. He noticed the mass while washing in the shower. He has had no pain, no weight loss, no change in sexual functioning, and no blood in his semen. Examination reveals the presence of a firm, nontender, 1 cm nodule on the testicle. No other masses and no inguinal adenopathy are noted. Ultrasound of the scrotum confirms that the mass is on the testicle.
What would be the next step in management?
A. 30-days of antibiotic for possible epididymitis followed by repeat examination
B. radical inguinal orchiectomy
C. needle biopsy of the mass
D. trans-scrotal orchiectomy
E. semen analysis and cytology for malignant cells
Correct Answer: B Section: (none)
Explanation:
A painless, firm testicular mass is a classic presentation of testicular cancer, although some men have pain or scrotal swelling as well. When such a mass is found on examination, ultrasound is the next indicated study to confirm whether the mass is truly located on the testicle or if it is associated with another structure, most commonly the epididymis. Once the presence is confirmed, an inguinal orchiectomy is the procedure of choice for both diagnostic and therapeutic purposes, as the vascular and lymphatic drainage of the testis is through the inguinal canal. Antibiotic therapy may play a role if the enlarged area is in the epididymis and not the testicle. Semen cytology plays no role in the work-up of suspected testicular malignancy
Question 599:
Numerous types of cancers are associated with infectious diseases. For which of the following cancers is there a vaccine currently available against the infectious agent which leads to the tumor?
A. Burkitt's lymphoma
B. gastric carcinoma
C. hepatocellular carcinoma
D. nasopharyngeal carcinoma
E. Kaposi's sarcoma
Correct Answer: C Section: (none)
Explanation:
Burkitt's lymphoma and nasopharyngeal carcinomas are associated with the Epstein-Barr virus. Gastric carcinoma is associated with H. pylori infection. Kaposi's sarcoma is associated with human herpesvirus 7. The rate of hepatocellular carcinoma is greatly increased in those with chronic hepatitis B and C. Hepatitis B virus infection is the leading cause of hepatocellular carcinoma worldwide, usually after congenital infection in Asia and Africa. Of these infections, only hepatitis B has a widely available, routinely recommended vaccine.
Question 600:
A32-year-old female presents for her first pap smear in more than 10 years. She has a history of heavy alcohol use and IV drug use and has performed sexual acts for drugs on numerous occasions. Testing performed today reveals her to have chlamydia cervicitis and trichomonas vaginalis and to be seropositive for hepatitis B and hepatitis C. HIV testing is negative. Her pap smear subsequently returns with carcinoma in-situ of the cervix.
Subsequent work-up confirms the presence of micro-invasive cervical carcinoma [Stage Ia]. What would be the most appropriate treatment?
A. simple hysterectomy
B. radical hysterectomy with pelvic lymph node dissection
C. cervical radiation therapy
D. cervical radiation followed by chemotherapy
E. hysterectomy followed by chemotherapy
Correct Answer: A Section: (none)
Explanation:
Human papillomavirus has been associated with the development of multiple squamous cell malignancies, including cervical cancer (HPV types 16, 18, 31, 45, and 5153), as well as anal, penile, and vulvar cancers. Recent evidence has also linked some oropharyngeal squamous cell cancers to HPV infection as well. The risk for HPV-associated cancer is increased in patients with HIV co-infection. HPV type 11 may cause genital warts but is not a likely cause of cervical cancer. The presence of other sexually transmitted diseases, such as Chlamydia or hepatitis B, may help to identify women at high risk for cervical cancer, but they are not direct causes of cervical cancer. Following the abnormal pap smear findings, the next step in the diagnosis of this patient would be a colposcopy with biopsy of any visualized cervical abnormalities. At this point, HPV testing and typing would not add to or change the work-up, so they would not be necessary. HPV testing and typing can be helpful in the evaluation of women with lower grade cervical cytological abnormalities, such as ASCUS. The other tests noted may be performed later in the diagnostic work-up, after the results of the biopsies are known.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.