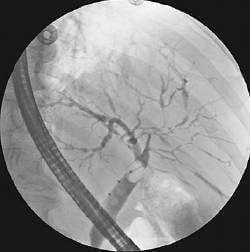
A42-year-old male with a history of ulcerative colitis has been to the ER three times over the past 6 months complaining of right upper quadrant pain, fever, and jaundice. His total bilirubin has fluctuated from 0.5 to
4.2 over this time. Workup has included an endoscopic retrograde cholangiopancreatography (ERCP) with the findings as shown in Figure. Of which of the following should the patient be informed?
A. The symptoms will resolve if he undergoes a total colectomy.
B. The only definitive treatment is liver transplantation.
C. Hepatic ultrasound is the best modality to diagnose his condition.
D. His disease is more commonly associated with irritable bowel syndrome.
E. A bacterial pathogen is the responsible agent.
Correct Answer: B Section: (none)
Explanation:
Sclerosing cholangitis is a chronic progressive disease of the liver in which an inflammatory process results in intrahepatic and/or extrahepatic biliary strictures. The disease is progressive and may eventually result in biliary cirrhosis and portal hypertension. Sclerosing cholangitis is strongly associated with ulcerative colitis and, to a lesser extent, with Crohn's disease. The precise cause is unknown; however, it has been suggested that it may result from a local response to viral infection. The diagnosis should be considered in a patient with inflammatory bowel disease who presents with abnormal liver function tests and a clinical picture of jaundice, intermittent right upper quadrant pain, nausea, vomiting, and fever. The diagnosis is traditionally established by ERCP demonstrating characteristic biliary strictures alternating with areas of dilatation that has been referred to as a "string of beads." The appropriate management of sclerosing cholangitis is supportive, with no known medical cure. Definitive treatment of the underlying ulcerative colitis with total colectomy does not prevent progression of the disease. In patients with diffuse and advanced parenchymal disease, hepatic transplantation is the only known cure.
Question 52:
Apatient is evaluated for left-sided abdominal pain and undergoes a CT scan of the abdomen that shows renal calculi. The radiologist reports an incidental finding that is shown in Figure. She has never been symptomatic from this disease. All of her hepatobiliary serologies are within normal limits. Which of the following is an indication for elective surgical treatment?
A. patient is over 50 years old
B. two small (<1 cm) stones and sludge present in gallbladder
C. absence of calcifications in the gallbladder wall
D. type II diabetes mellitus
E. sickle cell disease
Correct Answer: E Section: (none)
Explanation:
The incidental finding is a gallstone within the gallbladder without evidence for inflammation. For most patients with asymptomatic cholelithiasis, a cholecystectomy is not routinely performed. Only 2030% of these patients will develop symptoms within 20 years. Moreover, only 12% per year will develop serious symptoms or complications from their gallstones. However, certain patients are at greater risk for developing complications and should be considered for elective cholecystectomy. This population includes patients with stones greater than 2.5 cm in size since they are at greater risk for obstruction. Children with cholelithiasis have a high frequency of becoming symptomatic and also should be considered for early intervention. In patients with sickle cell disease, acute cholecystitis can induce a sickle crisis, which can complicate surgery and as such should undergo elective cholecystectomy. Finally, the finding of calcifications in the gallbladder wall, also known as a "porcelain gallbladder" is associated with increased risk of gallbladder carcinoma and an elective cholecystectomy should be considered. Diabetes mellitus is associated with increased surgical risks with both emergent and elective cholecystectomy, and therefore diabetics should not be recommended for surgery for asymptomatic gallstones.
Question 53:
You have been asked to see a patient of one of your colleagues. He is a 67-year-old male with a long smoking history who has been having left foot pain at night. He tells you that dangling his feet over the bed relieves the pain. Previously, he had noted pain in his left calf with ambulation. Over the past several weeks, this pain has been worsening and the distance he could walk pain free had diminished.
Which of the following is an indication for surgical revascularization?
A. pain in both calves when walking that relieves with rest
B. necrotic fifth toe
C. presence of a localized focus of arterial stenosis seen on angiogram
D. diabetic patient
E. patient refusal to consider quitting smoking, as he has a greater risk of disease progression
Correct Answer: B Section: (none)
Explanation:
The symptoms described by the patient are classic for rest pain. Patients often experience pain at night while lying in bed, and the pain improves with dependent positioning of the affected extremity. Initial evaluation of this patient should be an arterial duplex study of the vessels of the affected leg. This noninvasive test can provide great detail on the extent of the disease and the location of hemodynamically significant obstruction. Furthermore, it will help determine if inflow obstruction is present in the aorta or iliac vessels. It is crucial in these patients to determine if the arterial obstruction involves the aortoiliac vessels or is confined to the lower extremity vasculature. After determining the location of the atherosclerotic lesion, you can proceed with a traditional angiogram, CT angiogram, or even an MRI/MRA to evaluate the vessels in order to plan your intervention. The management of peripheral arterial occlusive disease is determined in part by the severity of the symptoms. Patients with limbthreatening ischemia, indicated by rest pain, tissue necrosis, and nonhealing wounds, should be considered for revascularization. On the other hand, patients with intermittent claudication, usually described as an "ache" in the calf, should first be managed conservatively. This includes institution of lifestyle modifications such as smoking cessation, walking programs, and medical therapy with pentoxifylline or cilostazol. However, patients with severe intermittent claudication that is lifestyle limiting should be considered for surgical revascularization.
Question 54:
You have been asked to see a patient of one of your colleagues. He is a 67-year-old male with a long smoking history who has been having left foot pain at night. He tells you that dangling his feet over the bed relieves the pain. Previously, he had noted pain in his left calf with ambulation. Over the past several weeks, this pain has been worsening and the distance he could walk pain free had diminished.
After a through history and physical examination, which of the following would be your next step in diagnostic workup?
A. three-view x-rays of his left foot and ankle
B. left lower extremity arterial duplex
C. lower extremity angiogram with runoff
D. trial of pentoxifylline with 3-month follow-up
E. CT angiogram to evaluate for aortoiliac occlusive disease
Correct Answer: B Section: (none)
Explanation:
The symptoms described by the patient are classic for rest pain. Patients often experience pain at night while lying in bed, and the pain improves with dependent positioning of the affected extremity. Initial evaluation of this patient should be an arterial duplex study of the vessels of the affected leg. This noninvasive test can provide great detail on the extent of the disease and the location of hemodynamically significant obstruction. Furthermore, it will help determine if inflow obstruction is present in the aorta or iliac vessels. It is crucial in these patients to determine if the arterial obstruction involves the aortoiliac vessels or is confined to the lower extremity vasculature. After determining the location of the atherosclerotic lesion, you can proceed with a traditional angiogram, CT angiogram, or even an MRI/MRA to evaluate the vessels in order to plan your intervention. The management of peripheral arterial occlusive disease is determined in part by the severity of the symptoms. Patients with limbthreatening ischemia, indicated by rest pain, tissue necrosis, and nonhealing wounds, should be considered for revascularization. On the other hand, patients with intermittent claudication, usually described as an "ache" in the calf, should first be managed conservatively. This includes institution of lifestyle modifications such as smoking cessation, walking programs, and medical therapy with pentoxifylline or cilostazol. However, patients with severe intermittent claudication that is lifestyle limiting should be considered for surgical revascularization.
Question 55:
A 64-year-old male is referred to your office for evaluation of a pulsatile abdominal mass. His primary care physician orders a CT scan of the abdomen and pelvis (see Figure). Which of the following is true regarding the finding illustrated on the CT?
A. 75% of patients with this have a positive family history for this condition.
B. Most patients with this will have aneurysms of peripheral vessels.
C. When this is greater than 4 cm in diameter it should be repaired.
D. Most are asymptomatic at presentation.
E. Endovascular repair should be restricted to young healthy patients.
Correct Answer: D Section: (none)
Explanation:
AAA is most common in the infrarenal aorta (shown by the arrow in Figure). Fifteen to twenty-five percent of patients with an AAAhave a first-degree relative with clinically apparent AAA. Fifteen percent of patients with an AAA will have an aneurysm of a peripheral vessel. Risk factors include age, gender, smoking, family history, and collagen vascular diseases such as Marfan syndrome. The risk of rupture of an AAA>5 cm is approximately 510% per year. At this point, the risk of rupture begins to outweigh the risk of open operative repair. Therefore, most patients with an aneurysm that has exceeded 5 cm in anteroposterior diameter should undergo repair. The role for endovascular repair of AAAcontinues to evolve. Recently, the benefits of this procedure in terms of decreased operative morbidity, mortality, length of stay, and recovery time
have been established while the long-term durability of this less invasive repair is still being evaluated. Endovascular repair has become a valuable tool in the treatment of AAA, but as the long-term outcomes are still uncertain, it is not yet the procedure of choice for young patients with this disease.
Question 56:
A 45-year-old woman, mother of four children, comes to the ER complaining of the sudden onset of epigastric and right upper quadrant pain, radiating to the back, associated with vomiting. On examination, tenderness is elicited in the right upper quadrant, bowel sounds are decreased, and laboratory data show leukocytosis as well as normal serum levels of amylase, lipase, and bilirubin Which of the following is the most useful diagnostic test to confirm the diagnosis?
A. two-way roentgenogram of the abdomen
B. ultrasonography of the upper abdomen
C. CT scan of the abdomen and pelvis with oral contrast
D. HIDA (hydroxy iminodiacetic acid) scan
E. magnetic resonance cholangiopancreatography (MRCP)
Correct Answer: B Section: (none)
Explanation:
Cholelithiasis is much more common in women than men. In addition to gender, the development of gallstones can also be affected by age, weight, family history, and pregnancy. Gallstones often remain asymptomatic, but they can cause symptoms when they cause obstruction of the cystic duct. The result of this obstruction is biliary colic, which is experienced as epigastric pain radiating to the back and can be associated with nausea and vomiting. The presence of tenderness to palpation in the right upper quadrant, fever, and leukocytosis would suggest acute cholecystitis, a complication of gallstones. In a patient suspected of having complications of gallstones, the best test for evaluation is ultrasonography. Ultrasonography is highly sensitive in detecting gallstones and also provides details about the thickness of the gallbladder wall, the presence of pericholecystic fluid, and also the presence or absence of tenderness over the gallbladder during the examination (sonographic Murphy's sign). A two-way roentgenogram of the abdomen is much less sensitive, detecting only 20% of gallstones. A CT scan of the abdomen with IV and PO contrast can be sensitive in detecting the inflammatory changes associated with acute cholecystitis, but it is much more expensive and time consuming when compared to ultrasound. A HIDA scan, although sensitive and specific in the right setting, is generally reserved for more complicated cases where the diagnosis is unclear. Failure to visualize the gallbladder with HIDA scan in 1 hour indicates either partial or complete cystic duct obstruction and confirms the diagnosis of acute cholecystitis. However, this should not be the first-line test in evaluating a patient for acute cholecystitis. Finally, an MRCP can be very useful in evaluating the biliary tree and the presence of choledocholithiasis in a patient with cholecystitis and an elevated bilirubin, but does not have a role in the diagnosis of acute cholecystitis
Question 57:
A 70-year-old male presents with dysphagia, regurgitation of undigested food, and halitosis. You obtain a barium swallow study (see Figure). Which of the following is true regarding this condition?
A. Esophagoscopy is a critical portion of the preoperative workup.
B. The diverticulum is situated posteriorly, just proximal to the cricopharyngeal muscle.
C. The diverticulum will involve all layers of the esophageal wall.
D. Treatment requires resection of the diverticulum.
E. Vocal cord paralysis is most likely secondary to a traumatic endotracheal intubation at the time of surgery.
Correct Answer: B Section: (none)
Explanation:
Pharyngoesophageal (Zenker's) diverticulum is the most common diverticulum of the esophagus, and is an example of a pulsion diverticulum. It is a false diverticulum and consists of the mucosa and submucosa protruding through the esophageal musculature. A true diverticulum would involve all three layers. It is situated posteriorly just proximal to the cricopharyngeal muscle, at a weak point in the esophagus. Symptoms include dysphagia, spontaneous regurgitation of undigested food/pills, noisy swallowing, and halitosis. The most serious complication of a Zenker's diverticulum is aspiration leading to pneumonia or a lung abscess. The diagnostic test of choice is a barium swallow. Both AP and lateral views are essential to estimate the size of the diverticulum and determine the side of deviation. Treatment mandates a cricopharyngeal myotomy in order to relieve the increased pressure at the upper esophageal sphincter that is responsible for the development of the diverticulum. Surgical management of the diverticulum itself could involve a resection or a diverticulopexy, which allows the pouch to spontaneously drain. Esophagoscopy with biopsy to rule out cancer is only indicated preoperatively if there is evidence of ulcers or mass defects on the barium swallow. EGD should be considered postoperatively because of a high association of GERD with Zenker's diverticula. Complications of surgery include infection, recurrence, vocal cord paralysis secondary to injury to the recurrent laryngeal nerve, and esophagocutaneous fistulas.
Question 58:
A 55-year-old female presents to your office after a lung mass was found on a chest x-ray. She has undergone a series of imaging studies and has been referred to your office to determine if she is a candidate for surgery. With which of the following findings would she still be a candidate for potentially curative surgical resection?
A. malignant pleural effusion
B. contralateral mediastinal node involvement
C. chest wall invasion
D. liver metastases
E. superior vena cava syndrome
Correct Answer: C Section: (none)
Explanation:
Tumor resectability in lung cancer is generally determined by (1) whether or not the resection is technically feasible and (2) whether or not the resection will result in improved survival. In general, invasion of the tumor into structures that are vital to life would classify the tumor as unresectable. For example, the presence of superior vena cava syndrome in the setting of lung cancer is generally the result of tumor growing into the superior vena cava, which cannot be surgically removed. Those patients should be treated with chemotherapy and radiation. For lung cancer, the presence of distant metastatic disease is a contraindication to surgical resection. Distant metastasis is defined by the presence of tumor in distant organs, such as brain, bone, or liver, as well as distant nodal involvement. In the treatment of lung cancer, this can be confusing when evaluating patients with lymph node metastases because the presence of positive ipsilateral medastinal nodes is not a contraindication to surgery, while positive contralateral mediastinal nodes indicates disseminated disease. With regards effusions, the presence of a pleural effusion in and of itself does not dictate the method of treatment, but identification of malignant cells within the effusion indicates noncurability and those patients should be treated medically. On the other hand, patients who present with local invasion of the tumor into the chest wall can potentially be cured of the disease with en bloc resection. Finally, involvement of more than one lobe has no bearing on prognosis as long as the patient's preoperative ventilation parameters will allow for safe resection.
Question 59:
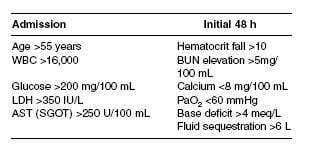
A 50-year-old male with a history of alcohol abuse presents with acute pancreatitis. Which of the following facts about the patient is included in Ranson's criteria?
A. age of 65 years old
B. elevated amylase
C. thrombocytosis
D. elevated lipase
E. evidence of pancreatic necrosis on CT scan
Correct Answer: A Section: (none)
Explanation:
Ranson's criteria represent a series of chemical clinical measurements that can be used to estimate the prognosis of an acute episode of pancreatitis. These markers are not meant for diagnosis of pancreatitis, but rather can be used to help gauge the severity of the disease and subsequently triage patients to the appropriate level of care. The criteria are measures of events that occur at admission and over the first 48 hours of hospitalization (see table below). Patients who meet three to four of the criteria have an estimated mortality of 15% and approximately 50% will require admission to the ICU. Essentially, all patients with five or more criteria will need to be cared for in the ICU, while patients with seven to eight positive criteria have a >90% mortality. It is important to note that amylase, lipase, and platelet counts are not considered in these criteria.
Question 60:
A 22-year-old male arrives in the trauma bay via ambulance. He was intubated in the field after suffering a gunshot wound to the head. On examination, he has both an entrance and exit wound suggesting a transcranial trajectory of the bullet. On physical examination, you note that there are no brain stem reflexes present and his pupils are fixed and dilated. Given his
A. Explain to them the process of organ transplantation and its benefits to others.
B. Withdraw mechanical ventilator support and allow the patient to expire.
C. Add a narcotic drip to the patient's treatment in order to ease his pain prior to withdrawing mechanical ventilation.
D. Contact the donor services agency to have a professional trained in addressing organ donation come to speak with the family.
E. Contact the transplant team and prepare the patient for the OR because the organs are too vital to waste regardless of the family's wishes.
Correct Answer: D Section: (none)
Explanation:
Organ donation can often be a very sensitive topic. As the transplant waiting lists continue to grow, the process of approaching the family of potential organ donors has been of great interest. In this setting, it is important to provide adequate information in a nonthreatening manner. Even today with donor cards, living wills, and so on, there can still be conflict between the patient and family, or even amongst family members, with regard organ transplantation. An individual who has been trained to discuss organ transplantation with grieving families best addresses this sensitive topic. Furthermore, regardless of the decision after appropriate discussions are held, it is vital to respect the family's choice.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.