A74-year-old male with a history of hypertension, CAD, and a 50 pack-year history of smoking presents with complaints of pain and cramping sensation of the thigh and buttock areas for the past 2 months. On detailed history, patient reports that the pain is usually during ambulation and relieves with sitting down. The pain does not change with respect to sitting or supine position. He denies any recent trauma, weakness of the legs, or paresthesias. He takes his prescription medications regularly and denies using alcohol, drugs, or any herbs/ supplements. Which of the following should be performed as an initial test to help confirm your clinical impression?
A. ankle-brachial index (ABI)
B. x-ray of the lumbar spine
C. electromyelography and nerve conduction studies of the lower extremities
D. lower extremity venous ultrasound with Dopplers
E. angiography of the aorta and lower extremities
Correct Answer: A Section: (none)
Explanation: Peripheral arterial disease (PAD) affects roughly 12% of the U.S. population with higher prevalence rates in persons over the age of 70. The classic symptoms of PAD are intermittent claudication which is usually described by patients as cramping pain in the calf, legs, thighs, or buttocks during any type of exercise that quickly relieves with rest. This scenario of worsening with activity and relief with rest is consistent with the disease process, as the pain results from ischemia. The ischemia is worse during periods of increased oxygen demand where the vascular insufficiency fails to meet the demand. Not all patients with PAD are symptomatic, thus an assessment of risk factors and a thorough physical examination are usually key to making the diagnosis in asymptomatic patients. The ABI is an easy, inexpensive, noninvasive test with a high correlation to angiography that can be done in the office. ABI is the usual initial test to screen for PAD.
A value of greater than 1.0 is considered normal, whereas values less than 0.9 are consistent with varying grades of PAD: · 1.0 or greater: normal · 0.810.9: mild PAD · 0.510.8: moderate PAD · <0.5: severe PAD The sensitivity of the ABI can be increased if performed post exercise. The ABI, however, has its limitations in patients with noncompressible, calcified vessels such as the elderly or in patients with diabetes. An ABI of greater than 1.3 may suggest the above scenario and its utility would be suspect. In these cases, more detailed testing may be warranted. Other modalities to assess PAD include arterial Dopplers, magnetic resonance angiography, and conventional angiography. The initial therapy for patients with PAD should be a trial of a structured walking program along with smoking cessation. Walking programs have been shown to increase walking distance without symptoms. In addition, walking also improves endothelial function, collateral vessel formation and function, and control of blood pressure, lipids, and blood sugars.
Pentoxyfylline has been traditionally recommended for PAD; however its efficacy is modest at best based on newer trial data. Antiplatelet agents may also be added for PAD as it will improve cardiovascular risk and perhaps modify the pathogenesis for PAD. Ultimately, risk factor modification is key for prevention and reduction of complications and comorbidities. Severe PAD or patients who require more specialized intervention may require vascular surgery consultation.
Question 642:
A 17-year-old male presents for evaluation of shortness of breath. He has episodes where he will audibly wheeze and have chest tightness. His symptoms worsen if he tries to exercise, especially when it is cold. He has used an OTC inhaler with good relief of his symptoms, but he finds that his symptoms are worsening. He now has episodes of wheezing on a daily basis and will have nighttime wheezing and coughing, on average, five or six times a month. You suspect a diagnosis of asthma.
Which of the following is the most appropriate pharmacologic regimen for this patient?
A. a systemic antihistamine as needed
B. a short-acting inhaled bronchodilator as needed
C. a scheduled inhaled steroid and a shortacting inhaled bronchodilator as needed
D. a scheduled long-acting beta agonist, a scheduled inhaled steroid, and a shortacting inhaled bronchodilator as needed
E. a systemic corticosteroid, a scheduled inhaled steroid, and a scheduled longacting beta agonist
Correct Answer: D Section: (none)
Explanation:
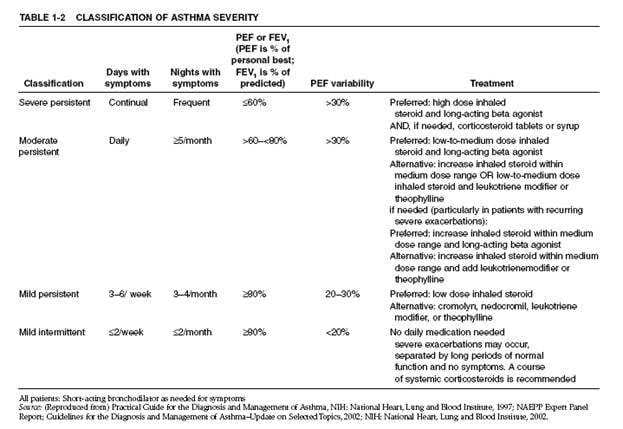
Asthma is a chronic lung disease characterized by inflammation of the airways, causing recurrent symptoms. The characteristic symptoms are wheezing, chest tightness, shortness of breath, or cough. Symptoms often worsen in the face of certain triggers, which include allergens, cold air, exercise, or other irritants. Physical examination may reveal hyperexpansion of the thorax, expiratory wheezing with a prolonged expiratory phase of respiration, and signs of allergies or atopic dermatitis. Asthma can be diagnosed by a history of episodic symptoms of airway obstruction (wheeze, dyspnea, cough, chest tightness), establishing the presence of airflow obstruction that is at least partially reversible and ruling out other causes of these symptoms/signs. Airflow obstruction can be shown by spirometry revealing an FEV1 of <80% predicted or an FEV1/forced vital capacity of <65% of the lower limit of normal. Reversibility can be shown by an FEV1 increase of 15% and at least 200 mL with the use of a short-acting beta agonist. Expiratory wheezing on examination is commonly seen in asthma but is a nonspecific finding. Many patients with asthma have elevated serum IgE levels; it is unusual to find asthma in individuals who have a low level of serum IgE. The sputum of asthmatics may contain eosinophils, Charcot-Leyden crystals, Curschmann spirals, or Creola bodies.
However, eosinophils may also be present in the sputum of patients with other conditions such as Churg-Strauss syndrome or eosinophilic pneumonia. Peak-flow monitoring is useful for the short-and long-term monitoring of asthma patients and for exacerbation management (by aiding in the determination of exacerbation severity which directs therapeutic decision making). persistent based on the frequency of symptoms and the degree of airflow obstruction. Based on this patient's frequency of symptoms, he falls into the moderate persistent class. An often neglected diagnosis is exerciseinduced asthma which is characterized by attacks immediately following exertion and by the lack of any long-term sequelae or increase in airway reactivity
Question 643:
A 17-year-old male presents for evaluation of shortness of breath. He has episodes where he will audibly wheeze and have chest tightness. His symptoms worsen if he tries to exercise, especially when it is cold. He has used an OTC inhaler with good relief of his symptoms, but he finds that his symptoms are worsening. He now has episodes of wheezing on a daily basis and will have nighttime wheezing and coughing, on average, five or six times a month. You suspect a diagnosis of asthma.
Your diagnostic workup confirms the diagnosis of asthma. What clinical classification of asthma does this patient have?
A. exercise-induced asthma
B. mild asthma
C. mild persistent asthma
D. moderate persistent asthma
E. severe persistent asthma
Correct Answer: D Section: (none)
Explanation:
Asthma is a chronic lung disease characterized by inflammation of the airways, causing recurrent symptoms. The characteristic symptoms are wheezing, chest tightness, shortness of breath, or cough. Symptoms often worsen in the face of certain triggers, which include allergens, cold air, exercise, or other irritants. Physical examination may reveal hyperexpansion of the thorax, expiratory wheezing with a prolonged expiratory phase of respiration, and signs of allergies or atopic dermatitis. Asthma can be diagnosed by a history of episodic symptoms of airway obstruction (wheeze, dyspnea, cough, chest tightness), establishing the presence of airflow obstruction that is at least partially reversible and ruling out other causes of these symptoms/signs. Airflow obstruction can be shown by spirometry revealing an FEV1 of <80% predicted or an FEV1/forced vital capacity of <65% of the lower limit of normal. Reversibility can be shown by an FEV1 increase of 15% and at least 200 mL with the use of a short-acting beta agonist. Expiratory wheezing on examination is commonly seen in asthma but is a nonspecific finding. Many patients with asthma have elevated serum IgE levels; it is unusual to find asthma in individuals who have a low level of serum IgE. The sputum of asthmatics may contain eosinophils, Charcot-Leyden crystals, Curschmann spirals, or Creola bodies.
However, eosinophils may also be present in the sputum of patients with other conditions such as Churg-Strauss syndrome or eosinophilic pneumonia. Peak-flow monitoring is useful for the short-and long-term monitoring of asthma patients and for exacerbation management (by aiding in the determination of exacerbation severity which directs therapeutic decision making). persistent based on the frequency of symptoms and the degree of airflow obstruction. Based on this patient's frequency of symptoms, he falls into the moderate persistent class. An often neglected diagnosis is exerciseinduced asthma which is characterized by attacks immediately following exertion and by the lack of any long-term sequelae or increase in airway reactivity
Question 644:
A 17-year-old male presents for evaluation of shortness of breath. He has episodes where he will audibly wheeze and have chest tightness. His symptoms worsen if he tries to exercise, especially when it is cold. He has used an OTC inhaler with good relief of his symptoms, but he finds that his symptoms are worsening. He now has episodes of wheezing on a daily basis and will have nighttime wheezing and coughing, on average, five or six times a month. You suspect a diagnosis of asthma. Which of the following would confirm your suspicion of the diagnosis of asthma?
A. presence of expiratory wheezing on examination
B. increase in FEV1 of 15% after giving inhaled albuterol
C. a decreased serum IgE level
D. presence of eosinophils on a sputum sample
E. a peak expiratory flow measurement 30% below the predicted normal value for the patient
Correct Answer: B Section: (none)
Explanation:
Asthma is a chronic lung disease characterized by inflammation of the airways, causing recurrent symptoms. The characteristic symptoms are wheezing, chest tightness, shortness of breath, or cough. Symptoms often worsen in the face of certain triggers, which include allergens, cold air, exercise, or other irritants. Physical examination may reveal hyperexpansion of the thorax, expiratory wheezing with a prolonged expiratory phase of respiration, and signs of allergies or atopic dermatitis. Asthma can be diagnosed by a history of episodic symptoms of airway obstruction (wheeze, dyspnea, cough, chest tightness), establishing the presence of airflow obstruction that is at least partially reversible and ruling out other causes of these symptoms/signs. Airflow obstruction can be shown by spirometry revealing an FEV1 of <80% predicted or an FEV1/forced vital capacity of <65% of the lower limit of normal. Reversibility can be shown by an FEV1 increase of 15% and at least 200 mL with the use of a short-acting beta agonist. Expiratory wheezing on examination is commonly seen in asthma but is a nonspecific finding. Many patients with asthma have elevated serum IgE levels; it is unusual to find asthma in individuals who have a low level of serum IgE. The sputum of asthmatics may contain eosinophils, Charcot-Leyden crystals, Curschmann spirals, or Creola bodies.
However, eosinophils may also be present in the sputum of patients with other conditions such as Churg-Strauss syndrome or eosinophilic pneumonia. Peak-flow monitoring is useful for the short-and long-term monitoring of asthma patients and for exacerbation management (by aiding in the determination of exacerbation severity which directs therapeutic decision making). persistent based on the frequency of symptoms and the degree of airflow obstruction. Based on this patient's frequency of symptoms, he falls into the moderate persistent class. An often neglected diagnosis is exerciseinduced asthma which is characterized by attacks immediately following exertion and by the lack of any long-term sequelae or increase in airway reactivity.
Question 645:
A 64-year-old male has been suffering from lower back pain for over 10 years. You have been following him for this period. You have prescribed stretching exercises and, occasionally, an anti-inflammatory medication to alleviate his pain. Although he has had no neurologic deficits in the past, today he has shown up in your office unexpectedly, complaining of bilateral lower back pain with numbness and tingling over the dorsal aspect of both feet. His symptoms have become progressively worse over the past 2 weeks and he is now unable to stand for more than 5 minutes without developing extreme pain and numbness. His symptoms are much improved by sitting down or kneeling over a chair. Climbing stairs seems to be tolerated well, but walking greatly exacerbates the pain. He denies bladder or bowel incontinence or retention, point tenderness or anesthesia in the lower back along the spinal cord or in the saddle area.
Which of the following imaging studies would be most helpful to confirm the diagnosis?
A. an MRI of the lumbosacral spine
B. an x-ray of the lumbosacral spine
C. an indium-tagged WBC scan
D. a bone scan of the sacrum
E. nerve conduction study of the legs bilaterally
Correct Answer: A Section: (none)
Explanation:
Although all of the given diagnoses could produce similar symptoms, there are distinct findings which suggest a diagnosis of spinal stenosis. Spinal stenosis is a degenerative disorder of the spine which normally presents after the age of 50. Neurologic symptoms, including dysesthesias and paraesthesias, and pain are often bilateral and not localized, since it commonly affects multiple vertebrae. The symptoms are improved with flexion of the spine (sitting or climbing stairs) and worsened by straightening the spine (standing). There is no localized pain in the sacrum and no bowel or bladder incontinence, so a diagnosis of cauda equina syndrome or spondyloarthopathy is less likely. Muscle spasms and early DJD should not produce such neurologic findings. The most sensitive and specific imaging study in the diagnosis of spinal stenosis, among those given above, is an MRI of the spine at the affected area. Although x-rays of the spine have been frequently used in the past in the evaluation of lower back pain, they have been shown to be of limited value in diagnosing pathology. Bone scans may detect malignancy or infection before radiography does, but are of no value in spinal stenosis. Indium scans would be useful in occult inflammatory pathology and nerve conduction studies would suggest a neuropathic deficit, but would not help in localizing the defect.
Question 646:
A 64-year-old male has been suffering from lower back pain for over 10 years. You have been following him for this period. You have prescribed stretching exercises and, occasionally, an anti-inflammatory medication to alleviate his pain. Although he has had no neurologic deficits in the past, today he has shown up in your office unexpectedly, complaining of bilateral lower back pain with numbness and tingling over the dorsal aspect of both feet. His symptoms have become progressively worse over the past 2 weeks and he is now unable to stand for more than 5 minutes without developing extreme pain and numbness. His symptoms are much improved by sitting down or kneeling over a chair. Climbing stairs seems to be tolerated well, but walking greatly exacerbates the pain. He denies bladder or bowel incontinence or retention, point tenderness or anesthesia in the lower back along the spinal cord or in the saddle area.
What is the likely diagnosis?
A. spondyloathropathy of the sacroiliac joint
B. age-related early degenerative joint disease (DJD) of the hips
C. spinal stenosis of the lumbosacral area
D. muscle spasm of the lower back
E. cauda equina syndrom
Correct Answer: C Section: (none)
Explanation: Although all of the given diagnoses could produce similar symptoms, there are distinct findings which suggest a diagnosis of spinal stenosis. Spinal stenosis is a degenerative disorder of the spine which normally presents after the age of 50. Neurologic symptoms, including dysesthesias and paraesthesias, and pain are often bilateral and not localized, since it commonly affects multiple vertebrae. The symptoms are improved with flexion of the spine (sitting or climbing stairs) and worsened by straightening the spine (standing). There is no localized pain in the sacrum and no bowel or bladder incontinence, so a diagnosis of cauda equina syndrome or spondyloarthopathy is less likely. Muscle spasms and early DJD should not produce such neurologic findings. The most sensitive and specific imaging study in the diagnosis of spinal stenosis, among those given above, is an MRI of the spine at the affected area. Although x-rays of the spine have been frequently used in the past in the evaluation of lower back pain, they have been shown to be of limited value in diagnosing pathology. Bone scans may detect malignancy or infection before radiography does, but are of no value in spinal stenosis. Indium scans would be useful in occult inflammatory pathology and nerve conduction studies would suggest a neuropathic deficit, but would not help in localizing the defect.
Question 647:
A 42-year-old woman with hyperlipidemia, hypertension, and hypothyroidism presents to your office for a routine follow-up visit. Her blood pressure is well controlled with hydrochlorothiazide. She has been on a stable dose of levothyroxine for 8 years and measurement of her TSH today is within normal limits. However, her LDL cholesterol level remains elevated despite taking a statin for the past 9 months and complying with lifestyle modifications. You decide that the addition of a low dose of cholestyramine would provide her with additional benefit. How would you advise the patient before beginning this therapy?
A. She should take other medications at least 1 hour before or 4 hours after cholestyramine.
B. She should take a multivitamin tablet daily.
C. She should ingest the cholestyramine in its dry form.
D. She may mix the cholestyramine with water, juices, or carbonated beverages.
E. She should discontinue the cholestyramine immediately if she experiences steatorrhea.
Correct Answer: A Section: (none)
Explanation:
Cholestyramine is a bile acid sequestrant which binds bile acids and similar steroids in the intestine, thereby reducing concentrations of LDLs in the circulation. Orally administered drugs may also bind to cholestyramine, however, impairing their efficacy by impairing absorption in the gut. This problem can be alleviated by administering other oral medications at least 1 hour before or 4 hours after cholestyramine. Examples of compounds which may be bound by cholestyramine include warfarin, digoxin, glipizide, phenytoin, methyldopa, thiazide diuretics, niacin, and statins. Fat-soluble vitamins (A, D, E, and K) may also bind to cholestyramine. Cholestyramine powder should never be administered in its dry form due to the risk of aspiration. It should be combined with water, pureed-consistency food, or a noncarbonated beverage. Use of carbonated liquids as a solvent may exacerbate the common side effects of heartburn and indigestion. Fat-soluble vitamins (A, D, E, and K) may also bind to cholestyramine; if steatorrhea develops, with associated impairment of fatsoluble vitamins, vitamin supplementation is recommended.
Question 648:
A 70-year-old male is seen in the office for chest pain. He reports that he is getting substernal chest pain, without radiation, when he mows his lawn. The pain resolves with 1015 minutes of rest. He has never had pain at rest. He has no other cardiac complaints and his review of systems is otherwise negative. He has an unremarkable medical history and takes only a baby aspirin a day. On examination, his blood pressure is 160/70, pulse 85, and respiratory rate 16. His cardiac examination is notable for a harsh, 3/6 systolic ejection murmur along the sternal border that radiates to the carotid arteries. His carotid pulsation is noted to rise slowly and is small and sustained. His lungs are clear. The remainder of his examination is normal.
Subsequent workup confirms the diagnosis of critical aortic stenosis. Which of the following treatments would be most appropriate at this time?
A. a beta-blocker
B. an ACE inhibitor
C. a long-acting nitrate with as-needed sublingual nitroglycerin
D. balloon valvuloplasty
E. aortic valve replacement
Correct Answer: E Section: (none)
Explanation:
Aortic stenosis is one of the most common valvular abnormalities found in adults. It can be congenital -such as a unicuspid or bicuspid valve--or acquired. In young adults, acquired aortic stenosis is often seen as a consequence of rheumatic fever. This is becoming less common in developed nations. In adults over the age of 65, the most common cause of aortic stenosis is age-related degenerative, calcific aortic stenosis. The valvular cusps are immobilized and the stenosis caused by calcium deposits along the flexion lines of the valves. Acquired aortic stenosis typically has a prolonged asymptomatic period. During this time the stenosis may be found incidentally by auscultation of the characteristic harsh, holosystolic murmur in the aortic valve area that radiates to the carotid arteries. There may also be a slow, small, and sustained arterial pulsation (pulsus parvus and tardus) due to the relative outflow obstruction. The cardinal symptoms of aortic stenosis that signal advancing disease, and increased risk of mortality, are angina, heart failure, and syncope. An ECG will show left ventricular hypertrophy in approximately 85% of symptomatic cases of aortic stenosis.
A normal ECG is possible but would be more likely in early, asymptomatic stages. S-T segment elevation would be more consistent with acute cardiac ischemia and Q waves would be more consistent with a completed MI. Low-voltage QRS complexes can be seen in several conditions, including pericardial effusion, COPD, or obesity. When considering the diagnosis of aortic stenosis, the initial diagnostic test of choice would be echocardiography. It would provide information on both the structure (bicuspid, tricuspid, and the like) and the function (valve area, pressures) of the valve. The size and function of the left ventricle can also be determined. If aortic stenosis is found on echocardiogram and the patient is symptomatic, the next test would be cardiac catheterization.
This would allow for direct measurement of the pressure gradient across the valve. It would also allow for evaluation of the status of the coronary arteries in order to determine whether CABG would need to be performed along with valve replacement. Exercise stress testing is relatively contraindicated in the setting of symptomatic aortic stenosis. Holter monitoring would only be useful if there were a concomitant arrhythmia. Electrophysiologic studies would not play a role in the typical evaluation of aortic stenosis.
Question 649:
A 70-year-old male is seen in the office for chest pain. He reports that he is getting substernal chest pain, without radiation, when he mows his lawn. The pain resolves with 1015 minutes of rest. He has never had pain at rest. He has no other cardiac complaints and his review of systems is otherwise negative. He has an unremarkable medical history and takes only a baby aspirin a day. On examination, his blood pressure is 160/70, pulse 85, and respiratory rate 16. His cardiac examination is notable for a harsh, 3/6 systolic ejection murmur along the sternal border that radiates to the carotid arteries. His carotid pulsation is noted to rise slowly and is small and sustained. His lungs are clear. The remainder of his examination is normal.
Which of the following would be the most appropriate test to order next?
A. echocardiogram
B. exercise stress test
C. cardiac catheterization
D. 24-hour Holter monitor
E. electrophysiologic studies
Correct Answer: A Section: (none)
Explanation:
Aortic stenosis is one of the most common valvular abnormalities found in adults. It can be congenital -such as a unicuspid or bicuspid valve--or acquired. In young adults, acquired aortic stenosis is often seen as a consequence of rheumatic fever. This is becoming less common in developed nations. In adults over the age of 65, the most common cause of aortic stenosis is age-related degenerative, calcific aortic stenosis. The valvular cusps are immobilized and the stenosis caused by calcium deposits along the flexion lines of the valves. Acquired aortic stenosis typically has a prolonged asymptomatic period. During this time the stenosis may be found incidentally by auscultation of the characteristic harsh, holosystolic murmur in the aortic valve area that radiates to the carotid arteries. There may also be a slow, small, and sustained arterial pulsation (pulsus parvus and tardus) due to the relative outflow obstruction. The cardinal symptoms of aortic stenosis that signal advancing disease, and increased risk of mortality, are angina, heart failure, and syncope. An ECG will show left ventricular hypertrophy in approximately 85% of symptomatic cases of aortic stenosis.
A normal ECG is possible but would be more likely in early, asymptomatic stages. S-T segment elevation would be more consistent with acute cardiac ischemia and Q waves would be more consistent with a completed MI. Low-voltage QRS complexes can be seen in several conditions, including pericardial effusion, COPD, or obesity. When considering the diagnosis of aortic stenosis, the initial diagnostic test of choice would be echocardiography. It would provide information on both the structure (bicuspid, tricuspid, and the like) and the function (valve area, pressures) of the valve. The size and function of the left ventricle can also be determined. If aortic stenosis is found on echocardiogram and the patient is symptomatic, the next test would be cardiac catheterization.
This would allow for direct measurement of the pressure gradient across the valve. It would also allow for evaluation of the status of the coronary arteries in order to determine whether CABG would need to be performed along with valve replacement. Exercise stress testing is relatively contraindicated in the setting of symptomatic aortic stenosis. Holter monitoring would only be useful if there were a concomitant arrhythmia. Electrophysiologic studies would not play a role in the typical evaluation of aortic stenosis.
Question 650:
A 70-year-old male is seen in the office for chest pain. He reports that he is getting substernal chest pain, without radiation, when he mows his lawn. The pain resolves with 1015 minutes of rest. He has never had pain at rest. He has no other cardiac complaints and his review of systems is otherwise negative. He has an unremarkable medical history and takes only a baby aspirin a day. On examination, his blood pressure is 160/70, pulse 85, and respiratory rate 16. His cardiac examination is notable for a harsh, 3/6 systolic ejection murmur along the sternal border that radiates to the carotid arteries. His carotid pulsation is noted to rise slowly and is small and sustained. His lungs are clear. The remainder of his examination is normal.
Which of the following would be most likely to be seen on an ECG?
A. S-T segment elevations in the precordial leads
B. Q waves in the precordial leads
C. low-voltage QRS complexes
D. left ventricular hypertrophy pattern
E. normal ECG
Correct Answer: D Section: (none)
Explanation:
Aortic stenosis is one of the most common valvular abnormalities found in adults. It can be congenital -such as a unicuspid or bicuspid valve--or acquired. In young adults, acquired aortic stenosis is often seen as a consequence of rheumatic fever. This is becoming less common in developed nations. In adults over the age of 65, the most common cause of aortic stenosis is age-related degenerative, calcific aortic stenosis. The valvular cusps are immobilized and the stenosis caused by calcium deposits along the flexion lines of the valves. Acquired aortic stenosis typically has a prolonged asymptomatic period. During this time the stenosis may be found incidentally by auscultation of the characteristic harsh, holosystolic murmur in the aortic valve area that radiates to the carotid arteries. There may also be a slow, small, and sustained arterial pulsation (pulsus parvus and tardus) due to the relative outflow obstruction. The cardinal symptoms of aortic stenosis that signal advancing disease, and increased risk of mortality, are angina, heart failure, and syncope. An ECG will show left ventricular hypertrophy in approximately 85% of symptomatic cases of aortic stenosis.
A normal ECG is possible but would be more likely in early, asymptomatic stages. S-T segment elevation would be more consistent with acute cardiac ischemia and Q waves would be more consistent with a completed MI. Low-voltage QRS complexes can be seen in several conditions, including pericardial effusion, COPD, or obesity. When considering the diagnosis of aortic stenosis, the initial diagnostic test of choice would be echocardiography. It would provide information on both the structure (bicuspid, tricuspid, and the like) and the function (valve area, pressures) of the valve. The size and function of the left ventricle can also be determined. If aortic stenosis is found on echocardiogram and the patient is symptomatic, the next test would be cardiac catheterization.
This would allow for direct measurement of the pressure gradient across the valve. It would also allow for evaluation of the status of the coronary arteries in order to determine whether CABG would need to be performed along with valve replacement. Exercise stress testing is relatively contraindicated in the setting of symptomatic aortic stenosis. Holter monitoring would only be useful if there were a concomitant arrhythmia. Electrophysiologic studies would not play a role in the typical evaluation of aortic stenosis.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.