A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees. There does not appear to be an arrhythmia present.
A transesophageal echocardiogram (TEE) is performed which reveals a left ventricular ejection fraction (LVEF) of 30%. Which of the following accurately describes this patient and his condition?
A. A transthoracic echocardiogram (TTE) would give a more accurate estimation of the patient's true LVEF.
B. He has diastolic heart failure.
C. Digoxin would be an appropriate choice in attempting to control symptoms.
D. He has class I heart failure according to the New York Heart Association (NYHA) classification.
E. Hypertension is the most common cause.
Correct Answer: C Section: (none)
Explanation:
This patient's presentation is most consistent with pulmonary edema from decompensated CHF. The BNP test has been found to be both sensitive and specific for the diagnosis of CHF. It can be a very useful test to order when a patient is dyspneic to help to determine if CHF is the cause. Troponin, CK-MB, and LDH are markers of damage to cardiac muscle and can be diagnostic in a MI. While MI can be a cause of CHF, and most patients presenting with CHF will have cardiac enzymes drawn as part of their evaluation, cardiac enzymes are neither sensitive nor specific for CHF. Similarly, a CXR can determine the presence of pulmonary edema but not its cause.
Acute pulmonary edema secondary to CHF will require management with diuresis for acute symptomatic relief. ACE inhibitors and beta-blockers do decrease mortality and morbidity in CHF; however their use in acute decompensated heart failure is suspected as they may induce hypotension and further cardiogenic shock. Digoxin is used for symptomatic relief either when other modalities fail or when rate control from atrial fibrillation is an issue. In patients with CHF and atrial fibrillation, beta-blockers have shown better effect and reduced morbidity than digoxin. Nevertheless, in the acute setting of decompensated heart failure with pulmonary edema, diuresis is the optimal initial treatment, not digoxin. In chronic heart failure, digoxin is reserved for patients with systolic failure that are symptomatic despite adequate ACE inhibitor and beta-blocker use. Furosemide is effective in treating the acute pulmonary edema associated with CHF by virtue of its potent diuretic action, which rapidly eliminates excess body fluid volume.
Question 652:
A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees. There does not appear to be an arrhythmia present. Which of the following has been shown to prolong survival in patients with this condition?
A. digoxin
B. nonsteroidal anti-inflammatory drugs(NSAIDs)
C. warfarin
D. carvedilol
E. diltiazem
Correct Answer: D Section: (none)
Explanation:
This patient's presentation is most consistent with pulmonary edema from decompensated CHF. The BNP test has been found to be both sensitive and specific for the diagnosis of CHF. It can be a very useful test to order when a patient is dyspneic to help to determine if CHF is the cause. Troponin, CK-MB, and LDH are markers of damage to cardiac muscle and can be diagnostic in a MI. While MI can be a cause of CHF, and most patients presenting with CHF will have cardiac enzymes drawn as part of their evaluation, cardiac enzymes are neither sensitive nor specific for CHF. Similarly, a CXR can determine the presence of pulmonary edema but not its cause.
Acute pulmonary edema secondary to CHF will require management with diuresis for acute symptomatic relief. ACE inhibitors and beta-blockers do decrease mortality and morbidity in CHF; however their use in acute decompensated heart failure is suspected as they may induce hypotension and further cardiogenic shock. Digoxin is used for symptomatic relief either when other modalities fail or when rate control from atrial fibrillation is an issue. In patients with CHF and atrial fibrillation, beta-blockers have shown better effect and reduced morbidity than digoxin. Nevertheless, in the acute setting of decompensated heart failure with pulmonary edema, diuresis is the optimal initial treatment, not digoxin. In chronic heart failure, digoxin is reserved for patients with systolic failure that are symptomatic despite adequate ACE inhibitor and beta-blocker use. Furosemide is effective in treating the acute pulmonary edema associated with CHF by virtue of its potent diuretic action, which rapidly eliminates excess body fluid volume.
Question 653:
A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees. There does not appear to be an arrhythmia present. Which of the following medications should be given initially?
A. metoprolol
B. diltiazem
C. furosemide
D. carvedilol
E. lisinopril
Correct Answer: C Section: (none)
Explanation:
This patient's presentation is most consistent with pulmonary edema from decompensated CHF. The BNP test has been found to be both sensitive and specific for the diagnosis of CHF. It can be a very useful test to order when a patient is dyspneic to help to determine if CHF is the cause. Troponin, CK-MB, and LDH are markers of damage to cardiac muscle and can be diagnostic in a MI. While MI can be a cause of CHF, and most patients presenting with CHF will have cardiac enzymes drawn as part of their evaluation, cardiac enzymes are neither sensitive nor specific for CHF. Similarly, a CXR can determine the presence of pulmonary edema but not its cause.
Acute pulmonary edema secondary to CHF will require management with diuresis for acute symptomatic relief. ACE inhibitors and beta-blockers do decrease mortality and morbidity in CHF; however their use in acute decompensated heart failure is suspected as they may induce hypotension and further cardiogenic shock. Digoxin is used for symptomatic relief either when other modalities fail or when rate control from atrial fibrillation is an issue. In patients with CHF and atrial fibrillation, beta-blockers have shown better effect and reduced morbidity than digoxin. Nevertheless, in the acute setting of decompensated heart failure with pulmonary edema, diuresis is the optimal initial treatment, not digoxin. In chronic heart failure, digoxin is reserved for patients with systolic failure that are symptomatic despite adequate ACE inhibitor and beta-blocker use. Furosemide is effective in treating the acute pulmonary edema associated with CHF by virtue of its potent diuretic action, which rapidly eliminates excess body fluid volume.
Question 654:
A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees. There does not appear to be an arrhythmia present.
Which test would be most sensitive for diagnosis of this condition?
A. troponin I
B. LDH
C. creatine kinase-MB isoenzyme (CK-MB)
D. brain natriuretic peptide (BNP)
E. CXR
Correct Answer: D Section: (none)
Explanation:
This patient's presentation is most consistent with pulmonary edema from decompensated CHF. The BNP test has been found to be both sensitive and specific for the diagnosis of CHF. It can be a very useful test to order when a patient is dyspneic to help to determine if CHF is the cause. Troponin, CK-MB, and LDH are markers of damage to cardiac muscle and can be diagnostic in a MI. While MI can be a cause of CHF, and most patients presenting with CHF will have cardiac enzymes drawn as part of their evaluation, cardiac enzymes are neither sensitive nor specific for CHF. Similarly, a CXR can determine the presence of pulmonary edema but not its cause.
Acute pulmonary edema secondary to CHF will require management with diuresis for acute symptomatic relief. ACE inhibitors and beta-blockers do decrease mortality and morbidity in CHF; however their use in acute decompensated heart failure is suspected as they may induce hypotension and further cardiogenic shock. Digoxin is used for symptomatic relief either when other modalities fail or when rate control from atrial fibrillation is an issue. In patients with CHF and atrial fibrillation, beta-blockers have shown better effect and reduced morbidity than digoxin. Nevertheless, in the acute setting of decompensated heart failure with pulmonary edema, diuresis is the optimal initial treatment, not digoxin. In chronic heart failure, digoxin is reserved for patients with systolic failure that are symptomatic despite adequate ACE inhibitor and beta-blocker use. Furosemide is effective in treating the acute pulmonary edema associated with CHF by virtue of its potent diuretic action, which rapidly eliminates excess body fluid volume.
Question 655:
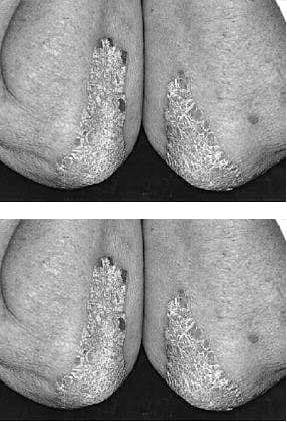
An 18-year-old female presents for follow-up of a rash. She states that she has been using OTC antifungal preparations without success. She used OTC cortisone cream with mild improvement, but the lesions never disappeared. Her condition also recurred with full severity once the cortisone cream was discontinued. Her family history reveals a first degree relative with similar rash. The rash is over the elbows, trunk, and scalp.
Which of the following would be the appropriate initial treatment?
A. methotrexate
B. systemic steroids
C. phototherapy
D. topical steroids
E. systemic biologicals
Correct Answer: D Section: (none)
Explanation:
Psoriasis is a benign chronic, inflammatory skin disorder with a genetic basis that affects approximately 2% of the population in the United States. The condition varies in its presentation from person to person, with some having only local involvement and others having a severe generalized involvement. The incidence occurs in a bimodal distribution, with peaks persons in their 20s and 50s. Those with earlier onset generally will have a more severe disease over the course of their lifetime. Psoriasis has several variants, or subtypes, including plaque type (most common), eruptive (guttate), generalized pustular, and erythrodermic psoriasis. Some patients may be asymptomatic or may have only minor itching. Others may have involvement of most of their body, with severe disfigurement and poor quality of life. Psoriasis may involve any skin area; however, areas such as the scalp, extensor surfaces, palms, soles, and nails should always be examined. The typical lesions are described as erythematous, well-demarcated plaques with overlying scales. Fine stippling (pitting) of the nails is highly suggestive of psoriasis. In addition to the skin findings, patients may also have arthritis. The lesions can be reactivated with local injury or irritation of normal skin (Koebner phenomenon). The diagnosis is predominantly clinical, based on the history and examination. There are no laboratory measures that will diagnose psoriasis. Skin biopsy, although not pathognomonic, would show features consistent with psoriasis and would help to rule out other similar appearing conditions.
Question 656:
An 18-year-old female presents for follow-up of a rash. She states that she has been using OTC antifungal preparations without success. She used OTC cortisone cream with mild improvement, but the lesions never disappeared. Her condition also recurred with full severity once the cortisone cream was discontinued. Her family history reveals a first degree relative with similar rash. The rash is over the elbows, trunk, and scalp .
Which of the following tests is most likely to confirm your clinical suspicion?
A. ESR and ANA
B. KOH prep and microscopic analysis of scraping from rash
C. biopsy of the involved area
D. capillary microscopy
E. Lyme titers
Correct Answer: C Section: (none)
Explanation:
Psoriasis is a benign chronic, inflammatory skin disorder with a genetic basis that affects approximately 2% of the population in the United States. The condition varies in its presentation from person to person, with some having only local involvement and others having a severe generalized involvement. The incidence occurs in a bimodal distribution, with peaks persons in their 20s and 50s. Those with earlier onset generally will have a more severe disease over the course of their lifetime. Psoriasis has several variants, or subtypes, including plaque type (most common), eruptive (guttate), generalized pustular, and erythrodermic psoriasis. Some patients may be asymptomatic or may have only minor itching. Others may have involvement of most of their body, with severe disfigurement and poor quality of life. Psoriasis may involve any skin area; however, areas such as the scalp, extensor surfaces, palms, soles, and nails should always be examined. The typical lesions are described as erythematous, well-demarcated plaques with overlying scales. Fine stippling (pitting) of the nails is highly suggestive of psoriasis. In addition to the skin findings, patients may also have arthritis. The lesions can be reactivated with local injury or irritation of normal skin (Koebner phenomenon). The diagnosis is predominantly clinical, based on the history and examination. There are no laboratory measures that will diagnose psoriasis. Skin biopsy, although not pathognomonic, would show features consistent with psoriasis and would help to rule out other similar appearing conditions.
Question 657:
An 18-year-old female presents for follow-up of a rash. She states that she has been using OTC antifungal preparations without success. She used OTC cortisone cream with mild improvement, but the lesions never disappeared. Her condition also recurred with full severity once the cortisone cream was discontinued. Her family history reveals a first degree relative with similar rash. The rash is over the elbows, trunk, and scalp .
Which other physical finding would be consistent with your presumptive diagnosis?
A. velvety, hyperpigmented patches over the axilla and neck
B. pitting of the nails
C. oily scalp
D. subcutaneous nodules
E. multiple tender and tense vesicles and bullae
Correct Answer: B Section: (none)
Explanation:
Psoriasis is a benign chronic, inflammatory skin disorder with a genetic basis that affects approximately 2% of the population in the United States. The condition varies in its presentation from person to person, with some having only local involvement and others having a severe generalized involvement. The incidence occurs in a bimodal distribution, with peaks persons in their 20s and 50s. Those with earlier onset generally will have a more severe disease over the course of their lifetime. Psoriasis has several variants, or subtypes, including plaque type (most common), eruptive (guttate), generalized pustular, and erythrodermic psoriasis. Some patients may be asymptomatic or may have only minor itching. Others may have involvement of most of their body, with severe disfigurement and poor quality of life. Psoriasis may involve any skin area; however, areas such as the scalp, extensor surfaces, palms, soles, and nails should always be examined. The typical lesions are described as erythematous, well-demarcated plaques with overlying scales. Fine stippling (pitting) of the nails is highly suggestive of psoriasis. In addition to the skin findings, patients may also have arthritis. The lesions can be reactivated with local injury or irritation of normal skin (Koebner phenomenon). The diagnosis is predominantly clinical, based on the history and examination. There are no laboratory measures that will diagnose psoriasis. Skin biopsy, although not pathognomonic, would show features consistent with psoriasis and would help to rule out other similar appearing conditions.
Question 658:
A 55-year-old male is brought to the ED, by ambulance, because of crushing chest pain radiating to his left shoulder and arm that started 1 hour ago. He has a history of hypertension, high cholesterol, and has smoked a pack of cigarettes a day for 30 years. He has never had symptoms like this before. Fortunately, the patient survives this episode. As part of his long-term treatment, which of the following would be an appropriate therapeutic intervention to initiate due to its proven effect on survival rate?
A. flecainide
B. captopril
C. quinidine
D. digoxin
E. nitroglycerin
Correct Answer: B Section: (none)
Explanation:
The clinical scenario described is classic for an acute MI. The patient has multiple risk factors, including smoking, hypertension, and elevated cholesterol. His symptoms of crushing chest pain radiating to the left arm is commonly seen in this setting. Often the first electrocardiographic sign of acute ischemia is the development of hyperacute T waves. The ECG will usually show S-T segment elevations in the area of the involved occluded vessel, with reciprocal S-T segment depressions in uninvolved areas. This can be followed by the eventual resolution of S-T segment abnormalities and the development of T wave inversions and Q waves. Diffuse P-R depressions are often the initial manifestation of pericarditis, a less common cause of acute chest pain. This often progresses to diffuse S-T segment elevations, the presence of which helps to distinguish pericarditis from the focal S-T elevations more classically associated with a thrombosed coronary artery. Q waves would be unlikely to occur within 1 hour of the onset of symptoms. In this clinical setting, a normal ECG, while possible, would be less likely to occur.
Ventricular arrhythmias, both tachycardia and fibrillation, are recognized complications of acute MI. The presence of ventricular fibrillation or pulseless ventricular tachycardia should lead to the primary "ABCD" survey, as outlined in the American Heart Association's ACLS protocols. The mnemonic stands for airway, breathing, circulation, and defibrillation. Epinephrine, lidocaine, or amiodarone are reserved for the setting where defibrillation is ineffective. Synchronized cardioversion would be used in efforts to convert a patient's rhythm in the setting of a stable tachycardia.
Question 659:
A 55-year-old male is brought to the ED, by ambulance, because of crushing chest pain radiating to his left shoulder and arm that started 1 hour ago. He has a history of hypertension, high cholesterol, and has smoked a pack of cigarettes a day for 30 years. He has never had symptoms like this before. The patient's rhythm converts to asystole. What is the most appropriate first action to take?
A. IV epinephrine
B. IV atropine
C. discontinuation of resuscitation
D. direct current (DC) cardioversion
E. check a second monitor lead
Correct Answer: E Section: (none)
Explanation:
The clinical scenario described is classic for an acute MI. The patient has multiple risk factors, including smoking, hypertension, and elevated cholesterol. His symptoms of crushing chest pain radiating to the left arm is commonly seen in this setting. Often the first electrocardiographic sign of acute ischemia is the development of hyperacute T waves. The ECG will usually show S-T segment elevations in the area of the involved occluded vessel, with reciprocal S-T segment depressions in uninvolved areas. This can be followed by the eventual resolution of S-T segment abnormalities and the development of T wave inversions and Q waves. Diffuse P-R depressions are often the initial manifestation of pericarditis, a less common cause of acute chest pain. This often progresses to diffuse S-T segment elevations, the presence of which helps to distinguish pericarditis from the focal S-T elevations more classically associated with a thrombosed coronary artery. Q waves would be unlikely to occur within 1 hour of the onset of symptoms. In this clinical setting, a normal ECG, while possible, would be less likely to occur.
Ventricular arrhythmias, both tachycardia and fibrillation, are recognized complications of acute MI. The presence of ventricular fibrillation or pulseless ventricular tachycardia should lead to the primary "ABCD" survey, as outlined in the American Heart Association's ACLS protocols. The mnemonic stands for airway, breathing, circulation, and defibrillation. Epinephrine, lidocaine, or amiodarone are reserved for the setting where defibrillation is ineffective. Synchronized cardioversion would be used in efforts to convert a patient's rhythm in the setting of a stable tachycardia.
Question 660:
A 55-year-old male is brought to the ED, by ambulance, because of crushing chest pain radiating to his left shoulder and arm that started 1 hour ago. He has a history of hypertension, high cholesterol, and has smoked a pack of cigarettes a day for 30 years. He has never had symptoms like this before.
While monitored in the ER, the patient's rhythm suddenly converts to ventricular tachycardia, and he becomes pulseless and unresponsive. Which of the following would be the most appropriate initial management of this situation?
A. defibrillation
B. synchronized cardioversion
C. IV amiodarone
D. IV lidocaine
E. IV epinephrine
Correct Answer: A Section: (none)
Explanation:
The clinical scenario described is classic for an acute MI. The patient has multiple risk factors, including smoking, hypertension, and elevated cholesterol. His symptoms of crushing chest pain radiating to the left arm is commonly seen in this setting. Often the first electrocardiographic sign of acute ischemia is the development of hyperacute T waves. The ECG will usually show S-T segment elevations in the area of the involved occluded vessel, with reciprocal S-T segment depressions in uninvolved areas. This can be followed by the eventual resolution of S-T segment abnormalities and the development of T wave inversions and Q waves. Diffuse P-R depressions are often the initial manifestation of pericarditis, a less common cause of acute chest pain. This often progresses to diffuse S-T segment elevations, the presence of which helps to distinguish pericarditis from the focal S-T elevations more classically associated with a thrombosed coronary artery. Q waves would be unlikely to occur within 1 hour of the onset of symptoms. In this clinical setting, a normal ECG, while possible, would be less likely to occur.
Ventricular arrhythmias, both tachycardia and fibrillation, are recognized complications of acute MI. The presence of ventricular fibrillation or pulseless ventricular tachycardia should lead to the primary "ABCD" survey, as outlined in the American Heart Association's ACLS protocols. The mnemonic stands for airway, breathing, circulation, and defibrillation. Epinephrine, lidocaine, or amiodarone are reserved for the setting where defibrillation is ineffective. Synchronized cardioversion would be used in efforts to convert a patient's rhythm in the setting of a stable tachycardia.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.