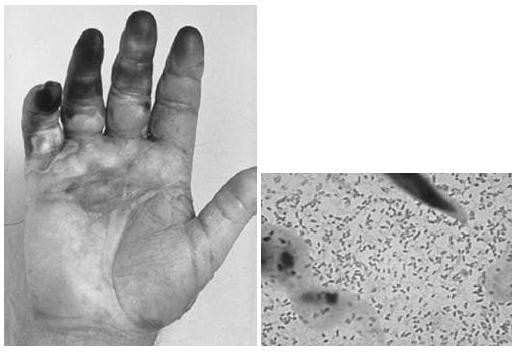
A 53-year-old fisherman develops pain and swelling of the right hand 8 hours after suffering a fish hook injury to the finger. On physical examination, the patient's temperature is 102.8°F and the patient ap pears septic. The patient's hand and a Gram stain of material aspirated from a bulla are shown in Figures below.
After appropriate wound care and debridement of necrotic tissue as necessary, which antibiotics should be started in this patient?
A. levofloxacin
B. vancomycin
C. doxycycline and ceftazidime
D. nafcillin and gentamicin
E. trimethoprim-sulfamethoxazole(TMP-SMZ)
Correct Answer: C Section: (none)
Explanation:
V. vulnificus is associated with sepsis in patients with liver disease who eat raw oysters or those with salt water contamination of wounds, like those caused by fish hooks. P. multocida is a cause of cellulitis caused by exposure to cat saliva as a result of a bite or a clawing injury. E. corrodens is associated with cellulitis caused by a human bite. Staphylococcus and Streptococcus are the most common causes of cellulitis. The Gram stain shows gram-negative, commashaped organisms typical for vibrios. Close attention should be paid to the wound site in the setting of a V. vulnificus infection. The wound site must be thoroughly cleaned and any necrotic tissue debrided. If necessary, fasciotomy or limb amputation should be performed. Antibiotic therapy should begin immediately as well. Use of a combination of doxycycline and a thirdgeneration cephalosporin such as ceftazidime is considered first-line. Quinolones may be considered as alternative therapy in the case of drug allergy or contraindication. A combination regimen using TMP-SMZ and an aminoglycoside is indicated for treatment in children since doxycycline and quinolones are contraindicated.
Question 732:
A 53-year-old fisherman develops pain and swelling of the right hand 8 hours after suffering a fish hook injury to the finger. On physical examination, the patient's temperature is 102.8°F and the patient ap pears septic. The patient's hand and a Gram stain of material aspirated from a bulla are shown in Figures below.
What is the most likely etiology of this bacteremia?
A. Staphylococcus aureus cellulitis
B. group A, beta-hemolytic Streptococcus sepsis
C. Pasteurella multocida cellulitis
D. Vibrio vulnificus sepsis
E. Eikenella corrodens cellulitis
Correct Answer: D Section: (none)
Explanation:
V. vulnificus is associated with sepsis in patients with liver disease who eat raw oysters or those with salt water contamination of wounds, like those caused by fish hooks. P. multocida is a cause of cellulitis caused by exposure to cat saliva as a result of a bite or a clawing injury. E. corrodens is associated with cellulitis caused by a human bite. Staphylococcus and Streptococcus are the most common causes of cellulitis. The Gram stain shows gram-negative, commashaped organisms typical for vibrios. Close attention should be paid to the wound site in the setting of a V. vulnificus infection. The wound site must be thoroughly cleaned and any necrotic tissue debrided. If necessary, fasciotomy or limb amputation should be performed. Antibiotic therapy should begin immediately as well. Use of a combination of doxycycline and a thirdgeneration cephalosporin such as ceftazidime is considered first-line. Quinolones may be considered as alternative therapy in the case of drug allergy or contraindication. A combination regimen using TMP-SMZ and an aminoglycoside is indicated for treatment in children since doxycycline and quinolones are contraindicated.
Question 733:
A 48-year-old woman complaining of dysuria is diagnosed with a UTI by urinalysis. Urine culture and sensitivities reveal that the causative organism belongs to the genus Klebsiella and is resistant to multiple antibiotics. Based upon the results available, you decide to begin therapy with gentamicin.
Which of the following would lead to the classification of this patient's infection as "complicated?"
A. a history of recurrent UTIs
B. a diagnosis of type II DM
C. the patient's gender
D. a history of undergoing a laparoscopic appendectomy 1 month ago
E. a postvoid residual volume of 25 cc
Correct Answer: B Section: (none)
Explanation:
Aminoglycosides such as gentamicin accumulate in the proximal tubular cells of the kidney, resulting in a defect in renal concentrating ability and reduced glomerular filtration after several days. This renal impairment is almost always reversible. Of all the aminoglycosides, gentamicin and tobramycin are the most nephrotoxic. Aminoglycosides may also cause ototoxicity in the form of irreversible auditory or vestibular damage. There is a direct relationship between aminoglycoside dosage and the risk for development of ototoxicity, so doses should be adjusted according to a patient's baseline renal function. Complicated UTIs involve metabolic or hormonal abnormalities such as those seen in M or during pregnancy; the presence of foreign bodies such as calculi, tumors, or catheters; the presence of strictures causing turbulent urine flow or vesicoureteral reflux; incomplete voiding such as that seen in neurogenic bladder, prostate hyperplasia or cancer; and, the presence of unusual infecting microorganisms. A history of recurrent UTI does not in itself lead to the classification of subsequent infections as complicated. Due to anatomic differences in urethral length between males and females, any UTI in a male is considered complicated. A history of recent surgery does not correlate with development of a complicated UTI unless the surgical procedure resulted in the creation of some anatomic abnormality which increased the risk of infection; examples of such abnormalities include adhesions or strictures. Apostvoid residual volume greater than 50100 mL suggests abnormal bladder emptying, which would predispose an individual to development of UTIs.
Question 734:
A 48-year-old woman complaining of dysuria is diagnosed with a UTI by urinalysis. Urine culture and sensitivities reveal that the causative organism belongs to the genus Klebsiella and is resistant to multiple antibiotics. Based upon the results available, you decide to begin therapy with gentamicin. Which of the following irreversible complications is also associated with gentamicin use?
A. vestibular dysfunction
B. cardiomyopathy
C. optic nerve dysfunction
D. myelodysplastic disease
E. cerebellar degeneration
Correct Answer: A Section: (none)
Explanation:
Aminoglycosides such as gentamicin accumulate in the proximal tubular cells of the kidney, resulting in a defect in renal concentrating ability and reduced glomerular filtration after several days. This renal impairment is almost always reversible. Of all the aminoglycosides, gentamicin and tobramycin are the most nephrotoxic. Aminoglycosides may also cause ototoxicity in the form of irreversible auditory or vestibular damage. There is a direct relationship between aminoglycoside dosage and the risk for development of ototoxicity, so doses should be adjusted according to a patient's baseline renal function. Complicated UTIs involve metabolic or hormonal abnormalities such as those seen in M or during pregnancy; the presence of foreign bodies such as calculi, tumors, or catheters; the presence of strictures causing turbulent urine flow or vesicoureteral reflux; incomplete voiding such as that seen in neurogenic bladder, prostate hyperplasia or cancer; and, the presence of unusual infecting microorganisms. A history of recurrent UTI does not in itself lead to the classification of subsequent infections as complicated. Due to anatomic differences in urethral length between males and females, any UTI in a male is considered complicated. A history of recent surgery does not correlate with development of a complicated UTI unless the surgical procedure resulted in the creation of some anatomic abnormality which increased the risk of infection; examples of such abnormalities include adhesions or strictures. Apostvoid residual volume greater than 50100 mL suggests abnormal bladder emptying, which would predispose an individual to development of UTIs.
Question 735:
A 48-year-old woman complaining of dysuria is diagnosed with a UTI by urinalysis. Urine culture and sensitivities reveal that the causative organism belongs to the genus Klebsiella and is resistant to multiple antibiotics. Based upon the results available, you decide to begin therapy with gentamicin.
Before doing so, you explain to the patient that antibiotics such as gentamicin are often associated with which of the following?
A. hepatotoxicity
B. nephrotoxicity
C. interstitial pulmonary fibrosis
D. pulmonary edema
E. splenomegaly
Correct Answer: B Section: (none)
Explanation:
Aminoglycosides such as gentamicin accumulate in the proximal tubular cells of the kidney, resulting in a defect in renal concentrating ability and reduced glomerular filtration after several days. This renal impairment is almost always reversible. Of all the aminoglycosides, gentamicin and tobramycin are the most nephrotoxic. Aminoglycosides may also cause ototoxicity in the form of irreversible auditory or vestibular damage. There is a direct relationship between aminoglycoside dosage and the risk for development of ototoxicity, so doses should be adjusted according to a patient's baseline renal function. Complicated UTIs involve metabolic or hormonal abnormalities such as those seen in M or during pregnancy; the presence of foreign bodies such as calculi, tumors, or catheters; the presence of strictures causing turbulent urine flow or vesicoureteral reflux; incomplete voiding such as that seen in neurogenic bladder, prostate hyperplasia or cancer; and, the presence of unusual infecting microorganisms. A history of recurrent UTI does not in itself lead to the classification of subsequent infections as complicated. Due to anatomic differences in urethral length between males and females, any UTI in a male is considered complicated. A history of recent surgery does not correlate with development of a complicated UTI unless the surgical procedure resulted in the creation of some anatomic abnormality which increased the risk of infection; examples of such abnormalities include adhesions or strictures. Apostvoid residual volume greater than 50100 mL suggests abnormal bladder emptying, which would predispose an individual to development of UTIs.
Question 736:
A 45-year-old male with type II diabetes, hypertension, and hyperlipidemia presents to your clinic as a new patient. He has been out of his cholesterol medications and came to your office requesting a refill. The patient brought his most recent lipid profile (done after he was off his cholesterol medication for 3 months) which revealed:
Cholesterol (total): 242 mg/dL HDL cholesterol: 38 mg/dL Triglycerides (TGs): 660 mg/dL LDL cholesterol = unable to calculate due to high TGs He also had recent liver function tests that were normal. Based on Adult Treatment Panel (ATP) III guidelines, which of the following medications should be the initial pharmacologic treatment for this patient?
A. atorvostatin
B. gemfibrozil
C. cholestyramine
D. omega-3 fatty acids
E. nicotinic acid
Correct Answer: B Section: (none)
Explanation:
According to the Third Report of the National Cholesterol Education Program (NCEP) on the ATP III once the TG levels are in very high range (>500 mg/dL) the focus changes from LDL to reducing TGs, as such high levels can trigger acute pancreatitis. Once the LDL is lower than 500 mg/dL, the attention can be turned toward lowering LDL for CHD reduction. The results of various recent meta-analyses revealed that elevated TGs are also an independent risk factor for CHD. Some factors that may lead to elevated TG include obesity, physical inactivity, tobacco use, alcohol use, high carbohydrate diets, diabetes, chronic kidney disease, familial disorders, and certain drugs. ATP III adopts the following classification for serum TGs: · Normal TGs: <150 mg/dL · Borderline-high TGs: 150199 mg/dL · High TGs: 200499 mg/dL · Very high TGs: 500 mg/dL Nicotinic acid and fibrates have the largest reduction in TG (2530% and 3550%, respectively) and are thus the first-line recommendations in addition to diet modification and exercise in cases of very high TG. Statins reduce TG by roughly 1033%, while bile acid sequestrant can have no effect or even increase TG levels. Fish oils in high doses can be used in recalcitrant cases as they may reduce TG by up to 50%; however GI side effects are common. It is also important to note that active omega-3 fatty acids make up only 3050% of many fish oil supplements, whereas Omacor has 90% omega-3 fatty acids. Although this class of agents can reduce TG effectively, they have the unwanted effect of elevating LDL-C levels.
Question 737:
A 35-year-old woman schedules an appointment in an outpatient clinic for evaluation and treatment of a "mouth problem." She says that she has white spots in her mouth that have been present for a few weeks. In response to your questioning, she states that she has been experiencing fatigue and a 20-lb weight loss over the past several months, although she attributes these symptoms to a dramatic increase in work hours at her job over the same period of time. She denies having any other chronic medical issues and does not use any prescription or OTC medications. As you examine her, you note the presence of white plaques on her buccal mucosa, palate, and tongue. Scraping of the plaques with a tongue depressor elicits pain as well as a small amount of bleeding. Nontender generalized cervical and submandibular lymphadenopathy is present.
Which of the following immunizations is safe to administer to this patient?
A. inactivated influenza vaccine
B. live attenuated influenza vaccine (FluMist)
C. varicella vaccine
D. oral polio vaccine (OPV)
E. measles mumps rubella (MMR) vaccine
Correct Answer: A Section: (none)
Explanation:
This patient's presenting symptoms are consistent with oropharyngeal candidiasis, or thrush. While risk factors for the development of thrush include recent antibiotic use, use of inhaled corticosteroids, and head or neck radiation, thrush is also commonly encountered in immunocompromised patients, such as those positive for HIV. Due to the patient's apparently benign prior medical history and the new onset of multiple complaints in addition to her oral candidal infection, an HIV infection should be considered. In order to assess a patient's risk for HIV exposure, a thorough history should be taken. Risk factors for HIV infection include unprotected sexual intercourse, multiple sexual partners, IV drug use, occupational exposure to blood or bodily fluids, blood transfusion prior to 1985, and use of nonsterile equipment in tattooing or body piercing. Generally, individuals positive for HIV should not receive live vaccines. Administration of inactivated influenza vaccine is recommended annually in all individuals positive for HIV. Live attenuated influenza vaccine was FDA approved in 2003 in an intranasal formulation but is contraindicated in individuals with immunocompromise. The varicella and MMR vaccines should not be administered to patients with severely symptomatic HIV infection. The OPV is no longer recommended for use in the United States despite its continued use in many other parts of the world. Instead, inactivated polio vaccine (IPV) is recommended and is safe for use in HIV-positive individuals.
Question 738:
A 35-year-old woman schedules an appointment in an outpatient clinic for evaluation and treatment of a "mouth problem." She says that she has white spots in her mouth that have been present for a few weeks. In response to your questioning, she states that she has been experiencing fatigue and a 20-lb weight loss over the past several months, although she attributes these symptoms to a dramatic increase in work hours at her job over the same period of time. She denies having any other chronic medical issues and does not use any prescription or OTC medications. As you examine her, you note the presence of white plaques on her buccal mucosa, palate, and tongue. Scraping of the plaques with a tongue depressor elicits pain as well as a small amount of bleeding. Nontender generalized cervical and submandibular lymphadenopathy is present.
Which of the following questions would potentially yield the most useful information in this patient's diagnosis and treatment?
A. "Do you have a family history of cancer?"
B. "Have you traveled outside of the country within the past 12 months?"
C. "Have you engaged in unprotected sexual intercourse?"
D. "Do you have any sick contacts?"
E. "How much do you smoke?"
Correct Answer: C Section: (none)
Explanation:
This patient's presenting symptoms are consistent with oropharyngeal candidiasis, or thrush. While risk factors for the development of thrush include recent antibiotic use, use of inhaled corticosteroids, and head or neck radiation, thrush is also commonly encountered in immunocompromised patients, such as those positive for HIV. Due to the patient's apparently benign prior medical history and the new onset of multiple complaints in addition to her oral candidal infection, an HIV infection should be considered. In order to assess a patient's risk for HIV exposure, a thorough history should be taken. Risk factors for HIV infection include unprotected sexual intercourse, multiple sexual partners, IV drug use, occupational exposure to blood or bodily fluids, blood transfusion prior to 1985, and use of nonsterile equipment in tattooing or body piercing. Generally, individuals positive for HIV should not receive live vaccines. Administration of inactivated influenza vaccine is recommended annually in all individuals positive for HIV. Live attenuated influenza vaccine was FDA approved in 2003 in an intranasal formulation but is contraindicated in individuals with immunocompromise. The varicella and MMR vaccines should not be administered to patients with severely symptomatic HIV infection. The OPV is no longer recommended for use in the United States despite its continued use in many other parts of the world. Instead, inactivated polio vaccine (IPV) is recommended and is safe for use in HIV-positive individuals.
Question 739:
A 31-year-old female health care worker presents to your clinic after a needlestick injury from a patient who subsequently left against medical advice prior to laboratory analysis for HIV or hepatitis. You advise your colleague that:
A. If the patient had HIV, her risk of seroconversion is 20%.
B. If the patient had Hepatitis B, her risk of seroconversion is 2%.
C. If the patient had Hepatitis C, her risk of seroconversion is 5%.
D. If the patient had HIV, her risk of seroconversion is 0.3%.
E. If the patient had Hepatitis C, her risk of seroconversion is 50%.
Correct Answer: D Section: (none)
Explanation:
The rate of HBV transmission to susceptible health care workers ranges from 6 to 30% after a single needlestick exposure to an HBV-positive patient. The average incidence of anti-HCV seroconversion after unintentional needle sticks or sharps exposure from an HCV-positive source is 1.8% (range, 07%). Average risk of HIV transmission after a percutaneous exposure to HIV-infected blood is approximately 0.3%. Postexposure prophylaxis may reduce the risk of transmission of HIV following a needlestick.
Question 740:
A 76-year-old alcoholic male with hypertension, type II diabetes, and a history of congestive heart presented with cough, fever, malaise, and chills. His initial vitals were: HR 110, T: 102°F, RR: 25, B P 90/60, O2 saturation 93% on 4L/NC. The patient decompensated in the ER and was intubated. Intubation was achieved after three attempts secondary to patient vomiting during the initial attempts. Patient was admitted to the ICU with a diagnosis of sepsis and respiratory failure secondary to suspected pneumonia. After obtaining blood and sputum cultures, the initial empiric antibiotic coverage should be which of the following?
A. gatifloxacin alone
B. vancomycin and metronidazole
C. ceftriaxone and azithromycin
D. ceftriaxone, gatifloxacin, and azithromycin
E. ampicillin/sulbactam and gatifloxacin
Correct Answer: E Section: (none)
Explanation:
Patients with pneumonia who are admitted to the ICU should be given empiric antibiotic coverage once the cultures are sent. According to the guidelines set forth by the Infectious Disease Society of America, empiric antibiotic coverage could be initiated with any of the following:
This patient is at high risk for aspiration because of his vomiting and history of alcoholism. Thus, choice E would be the most appropriate initial regimen in order to cover gram-positive, gram-negative, atypical, and anaerobic pathogens. The ampicillin-sulbactam covers gram positive, negative, and anaerobes. The flouroquinolone adds the atypical coverage in addition to providing gram-positive/ -negative coverage.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.