A 24-year-old male presents with sore throat, subjective fever, abdominal pain, and bad breath. He says that a neighbor's child is currently being treated for strep throat. On examination, his temperature is 101.1° F and his other vital signs are normal. He appears well. His throat is erythematous and his tonsils are enlarged, but there are no pharyngeal or tonsillar exudates. He has no cervical adenopathy. He has an occasional cough but his lungs are clear. His abdominal examination is normal. The presence of which of the following findings is a clinical predictor for the diagnosis of streptococcal pharyngitis?
A. erythematous tonsils
B. cough
C. tonsillar exudates
D. posterior cervical lymphadenopathy
E. halitosis
Correct Answer: C Section: (none)
Explanation: Pharyngitis is a commonly encountered problem in primary care. Patients with upper respiratory symptoms are often convinced that they need antibiotics. Often the etiology is viral, but ruling out bacterial etiology is crucial as the secondary complications can be severe. In terms of group Astrep pharyngitis, it is often difficult to make a clinical diagnosis based on one or two factors. Many studies have been performed to guide the clinician in making an empiric diagnosis of group A strep pharyngitis. Fever, tonsillar exudates, tender anterior cervical lymphadenopathy, absence of cough and tonsillar hypertrophy are all positive predictors. A patient who has at least two of these criteria should have a rapid strep test or culture--with treatment initiated if the test is positive. When a patient meets three or more criteria and is ill appearing, empiric treatment may be justified. If the patient has a negative rapid strep test and the clinician is suspicious, empiric treatment may be started and throat culture should be obtained. Apatient with a positive culture or rapid strep test should be treated, but a test of cure does not need to be performed. The throat culture has a sensitivity of 97% and specificity of 99%, while the rapid strep test has a sensitivity of 8097% and a specificity of >95%.
Question 752:
A 72-year-old diabetic is transferred to your hospital for fever and altered mental status in the late summer.
Symptoms started in this patient 1 week prior to admission. On physical examination, the patient was
disoriented. There were no focal neurologic findings. There was a fine rash on the patient's trunk. On oral
examination, there were tongue fasciculations. A lumbar puncture was performed which showed a glucose
of 71 and a protein of 94; microscopy of the cerebrospinal fluid (CSF) revealed 9 RBC and 14 WBC (21 P,
68 L, 11 H). The creatinine phosphokinase was 506. An electroencephalogram and MRI of the brain were
normal.
What further diagnostic test is the most appropriate?
A. Perform a West Nile virus IgM on the CSF.
B. Perform a serum cryptococcal antigen.
C. Perform C. immitis complement fixation tests.
D. Perform a sinus series.
E. Perform a purified protein derivative (PPD) skin test.
Correct Answer: A Section: (none)
Explanation:
This is a clinical presentation of West Nile virus infection. The tongue fasciculations go along with an inflammation at the base of the brain. The patient is at the right age for West Nile virus infection and he is immunocompromised due to diabetes. The diagnosis can be made by performing a West Nile virus IgM titer on the CSF. Diabetics can have cryptococcal meningitis. Lumbar puncture in this setting is usually normal with increased opening pressure, and rhabdomyolysis is not a feature of this disease. Diabetics are more at risk for candidiasis. However, the patient has no history of instrumentation, IV catheters, or other situations that would lead to disseminated candidiasis. Diabetics are at increased risk for C. immitis infection, but we have no history of the patient living in an area endemic for this organism. Diabetics are at increased risk for rhinocerebral mucormycosis. An MRI of the head might have shown involvement of the sinus. However, this patient's presentation is not consistent with rhinocerebral mucormycosis.
Question 753:
A 72-year-old diabetic is transferred to your hospital for fever and altered mental status in the late summer. Symptoms started in this patient 1 week prior to admission. On physical examination, the patient was disoriented. There were no focal neurologic findings. There was a fine rash on the patient's trunk. On oral examination, there were tongue fasciculations. A lumbar puncture was performed which showed a glucose of 71 and a protein of 94; microscopy of the cerebrospinal fluid (CSF) revealed 9 RBC and 14 WBC (21 P, 68 L, 11 H). The creatinine phosphokinase was 506. An electroencephalogram and MRI of the brain were normal. What is the best interpretation of these findings?
A. The patient may have cryptococcal meningitis.
B. The patient may have disseminated candidiasis.
C. The patient may have West Nile virus.
D. The patient may have Coccidioides immitis infection.
E. The patient may have rhinocerebral mucormycosis.
Correct Answer: C Section: (none)
Explanation:
This is a clinical presentation of West Nile virus infection. The tongue fasciculations go along with an inflammation at the base of the brain. The patient is at the right age for West Nile virus infection and he is immunocompromised due to diabetes. The diagnosis can be made by performing a West Nile virus IgM titer on the CSF. Diabetics can have cryptococcal meningitis. Lumbar puncture in this setting is usually normal with increased opening pressure, and rhabdomyolysis is not a feature of this disease. Diabetics are more at risk for candidiasis. However, the patient has no history of instrumentation, IV catheters, or other situations that would lead to disseminated candidiasis. Diabetics are at increased risk for C. immitis infection, but we have no history of the patient living in an area endemic for this organism. Diabetics are at increased risk for rhinocerebral mucormycosis. An MRI of the head might have shown involvement of the sinus. However, this patient's presentation is not consistent with rhinocerebral mucormycosis.
Question 754:
Apatient you see routinely in the clinic has elevated liver function tests. ALT is 89, AST is 75, and the total bilirubin and alkaline phosphatase are normal. The patient has no past history of hepatitis, taking medications, or excessive drinking. You order hepatitis serologies. The results are as follows: Positive: HBsAg and anti-HBc. Negative: anti-HBs, anti-HBc IgM, anti-HAV, and anti-HCV Which statement best describes this clinical situation?
A. If the patient was found to be HBe antigen positive, he would be considered highly infectious to spread hepatitis B.
B. This patient is in the "window period" because the antibody to hepatitis BsAg is negative.
C. This patient is not at risk for delta hepatitis because the patient has antibody to hepatitis B core.
D. The low level of transaminase elevations indicates that this patient is not a candidate for hepatitis B antiviral treatment.
E. If this patient has antibody to hepatitis Be, he is a candidate for antiviral therapy.
Correct Answer: A Section: (none)
Explanation:
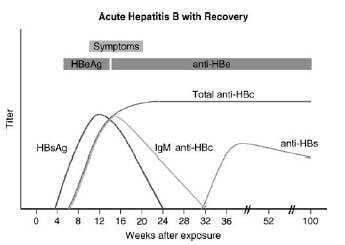
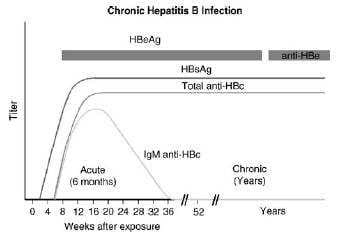
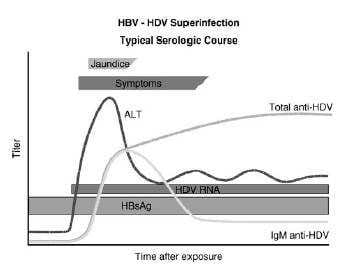
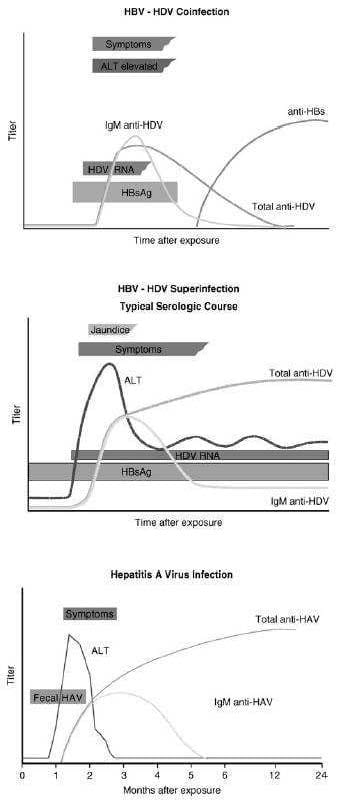
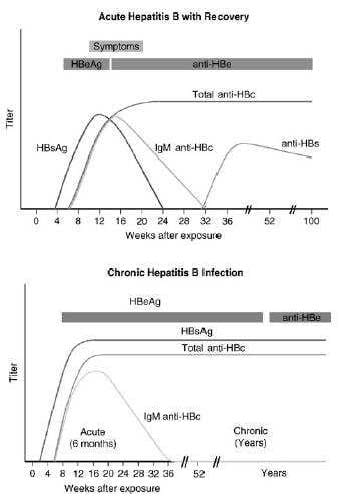
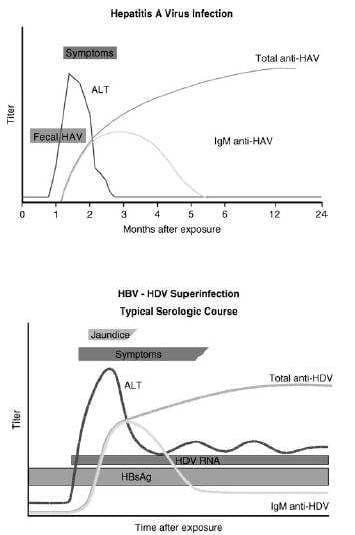
This patient has chronic hepatitis B. The different serologic studies for hepatitis B are shown in two figures below. The patient does not have acute hepatitis B because the IgM antibody to hepatitis B core is negative, and the total antibody to hepatitis B core is positive. Antibody to hepatitis B core occurs prior to the development of antibody to hepatitis B surface. IgM is found in acute infections; primarily IgG is seen in chronic infections.
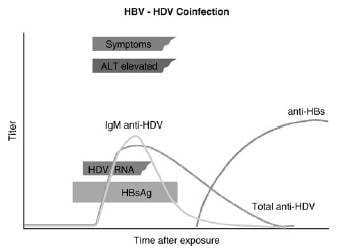
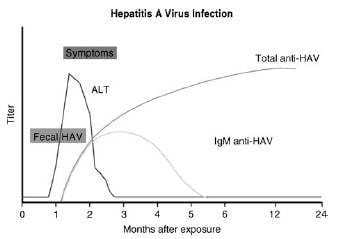
The presence of antibody to hepatitis B core with a positive hepatitis B surface antigen is indicative of chronic infection. Delta hepatitis infection requires the hepatitis B surface antigen. Delta hepatitis can occur concurrently with acute hepatitis B infection or later in the setting of chronic hepatitis B infection. There is no test for hepatitis C antigen. This is not a presentation of acute hepatitis A, which usually has very high transaminases. The antibody to hepatitis A virus occurs after 1 month and is associated with high transaminases Hepatitis Avaccine is indicated for patients with chronic liver disease. If this patient had hepatitis C, then hepatitis B vaccine would also be indicated. Hepatitis B vaccine is essentially hepatitis B surface antigen that causes the production of hepatitis B surface antibody. Since this patient has hepatitis B surface antigen already, choice C would be incorrect. Verifying the diagnosis with a qualitative hepatitis B viral load is not necessary. A quantitative hepatitis B viral load might be useful to evaluate for potential antiviral therapy. The only reason hepatitis Awould be recommended for the patient's spouse would be if the patient had acute hepatitis A. Investigating for other causes of hepatitis is not necessary as the diagnosis of chronic hepatitis B is already established. If the patient was found to be HBeAg positive, he would be considered highly infectious for the spread of hepatitis B. Hepatitis Be antigen is the DNA polymerase that shows active replication of the hepatitis B virion. These patients are 100 times more infectious than those lacking the hepatitis Be antigen. The window period is a situation where a patient is just recovering from hepatitis B. Hepatitis Bs antigen is negative and the antibody to hepatitis Bs has not been developed. The diagnosis is made by antibody to hepatitis B core. This is seen in Figure 1-6. Any patient who is hepatitis B surface antigen positive is at risk for delta hepatitis. This patient would be at risk for delta hepatitis by virtue of having a positive hepatitis B surface antigen. There is no level of transaminases, even normal transaminases, which would preclude antiviral therapy. The level of viral production indicated by the hepatitis B quantitative viral load, along with an assessment of the underlying liver pathology, is the best indication of need for treatment. As mentioned earlier, the antibody to hepatitis B would show the patient is less infectious and likely have a lower viral load.
Question 755:
Apatient you see routinely in the clinic has elevated liver function tests. ALT is 89, AST is 75, and the total bilirubin and alkaline phosphatase are normal. The patient has no past history of hepatitis, taking medications, or excessive drinking. You order hepatitis serologies. The results are as follows: Positive: HBsAg and anti-HBc. Negative: anti-HBs, anti-HBc IgM, anti-HAV, and anti-HCV
What is the most appropriate next step for this patient?
A. Verify the diagnosis with a qualitative hepatitis B viral load.
B. Vaccinate the patient with hepatitis A vaccine.
C. Vaccinate the patient with hepatitis B vaccine.
D. Investigate other causes of hepatitis, such as cytomegalovirus (CMV) and Epstein-Barr virus.
E. Recommend the patient's spouse receive hepatitis A vaccine.
Correct Answer: B Section: (none)
Explanation:
This patient has chronic hepatitis B. The different serologic studies for hepatitis B are shown in two figures below. The patient does not have acute hepatitis B because the IgM antibody to hepatitis B core is negative, and the total antibody to hepatitis B core is positive. Antibody to hepatitis B core occurs prior to the development of antibody to hepatitis B surface. IgM is found in acute infections; primarily IgG is seen in chronic infections.
The presence of antibody to
hepatitis B core with a positive hepatitis B surface antigen is indicative of chronic infection. Delta hepatitis infection requires the hepatitis B surface antigen. Delta hepatitis can occur concurrently with acute hepatitis B infection or later in the setting of chronic hepatitis B infection. There is no test for hepatitis C antigen. This is not a presentation of acute hepatitis A, which usually has very high transaminases. The antibody to hepatitis A virus occurs after 1 month and is associated with high transaminases Hepatitis Avaccine is indicated for patients with chronic liver disease. If this patient had hepatitis C, then hepatitis B vaccine would also
be indicated. Hepatitis B vaccine is essentially hepatitis B surface antigen that causes the production of hepatitis B surface antibody. Since this patient has hepatitis B surface antigen already, choice C would be incorrect. Verifying the diagnosis with a qualitative hepatitis B viral load is not necessary. A quantitative hepatitis B viral load might be useful to evaluate for potential antiviral therapy. The only reason hepatitis Awould be recommended for the patient's spouse would be if the patient had acute hepatitis A. Investigating for other causes of hepatitis is not necessary as the diagnosis of chronic hepatitis B is already established.
If the patient was found to be HBeAg positive, he would be considered highly infectious for the spread of hepatitis B. Hepatitis Be antigen is the DNA polymerase that shows active replication of the hepatitis B virion. These patients are 100 times more infectious than those lacking the hepatitis Be antigen. The window period is a situation where a patient is just recovering from hepatitis B. Hepatitis Bs antigen is negative and the antibody to hepatitis Bs has not been developed. The diagnosis is made by antibody to hepatitis B core. This is seen in Figure 1-6. Any patient who is hepatitis B surface antigen positive is at risk for delta hepatitis. This patient would be at risk for delta hepatitis by virtue of having a positive hepatitis B surface antigen. There is no level of transaminases, even normal transaminases, which would preclude antiviral therapy. The level of viral production indicated by the hepatitis B quantitative viral load, along with an assessment of the underlying liver pathology, is the best indication of need for treatment. As mentioned earlier, the antibody to hepatitis B would show the patient is less infectious and likely have a lower viral load.
Question 756:
Apatient you see routinely in the clinic has elevated liver function tests. ALT is 89, AST is 75, and the total bilirubin and alkaline phosphatase are normal. The patient has no past history of hepatitis, taking medications, or excessive drinking. You order hepatitis serologies. The results are as follows: Positive: HBsAg and anti-HBc. Negative: anti-HBs, anti-HBc IgM, anti-HAV, and anti-HCV
What is your interpretation?
A. The patient has acute hepatitis B.
B. The patient needs a test for IgM antibody to hepatitis A virus to rule out acute hepatitis A.
C. The patient needs a test for hepatitis C antigen to exclude acute hepatitis C.
D. The patient has chronic hepatitis B.
E. If the patient had a negative test for HBsAg, they could be infected with hepatitis delta.
Correct Answer: D Section: (none)
Explanation:
This patient has chronic hepatitis B. The different serologic studies for hepatitis B are shown in two figures below. The patient does not have acute hepatitis B because the IgM antibody to hepatitis B core is negative, and the total antibody to hepatitis B core is positive. Antibody to hepatitis B core occurs prior to the development of antibody to hepatitis B surface. IgM is found in acute infections; primarily IgG is seen in chronic infections.
The presence of antibody to hepatitis B core with a positive hepatitis B surface antigen is indicative of chronic infection. Delta hepatitis infection requires the hepatitis B surface antigen. Delta hepatitis can occur concurrently with acute hepatitis B infection or later in the setting of chronic hepatitis B infection. There is no test for hepatitis C antigen. This is not a presentation of acute hepatitis A, which usually has very high transaminases. The antibody to hepatitis A virus occurs after 1 month and is associated with high transaminases Hepatitis Avaccine is indicated for patients with chronic liver disease. If this patient had hepatitis C, then hepatitis B vaccine would also be indicated. Hepatitis B vaccine is essentially hepatitis B surface antigen that causes the production of hepatitis B surface antibody. Since this patient has hepatitis B surface antigen already, choice C would be incorrect. Verifying the diagnosis with a qualitative hepatitis B viral load is not necessary. A quantitative hepatitis B viral load might be useful to evaluate for potential antiviral therapy. The only reason hepatitis Awould be recommended for the patient's spouse would be if the patient had acute hepatitis A. Investigating for other causes of hepatitis is not necessary as the diagnosis of chronic hepatitis B is already established.
If the patient was found to be HBeAg positive, he would be considered highly infectious for the spread of hepatitis B. Hepatitis Be antigen is the DNA polymerase that shows active replication of the hepatitis B virion. These patients are 100 times more infectious than those lacking the hepatitis Be antigen. The window period is a situation where a patient is just recovering from hepatitis B. Hepatitis Bs antigen is negative and the antibody to hepatitis Bs has not been developed. The diagnosis is made by antibody to hepatitis B core. This is seen in Figure 1-6. Any patient who is hepatitis B surface antigen positive is at risk for delta hepatitis. This patient would be at risk for delta hepatitis by virtue of having a positive hepatitis B surface antigen. There is no level of transaminases, even normal transaminases, which would preclude antiviral therapy. The level of viral production indicated by the hepatitis B quantitative viral load, along with an assessment of the underlying liver pathology, is the best indication of need for treatment. As mentioned earlier, the antibody to hepatitis B would show the patient is less infectious and likely have a lower viral load.
Question 757:
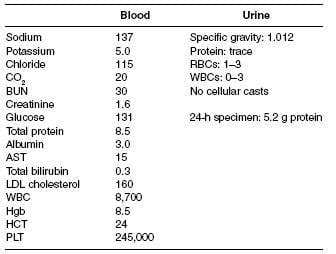
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows:
Which of the following microscopic findings on kidney biopsy is most usually associated with HIV infection?
A. pauci-immune crescentic glomerulonephritis
B. focal segmental glomerulosclerosis (collapsing variant)
C. membranous nephropathy
D. membranoproliferative glomerulonephritis
E. anti-GBM disease
Correct Answer: B Section: (none)
Explanation:
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti-GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Question 758:
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows:
Which of the following antihypertensive medications would be best implemented in patients with diabetic nephropathy?
A. lisinopril 10 mg orally once daily
B. clonidine 0.2 mg orally twice daily
C. metoprolol 25 mg orally twice daily
D. amlodipine 5 mg orally once daily
E. hydralazine 25 mg orally three times daily
Correct Answer: A Section: (none)
Explanation:
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti-GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Question 759:
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows: Which additional of the following would best help in the determination of the etiology of this patient's nephrotic syndrome?
A. fractional excretion of sodium
B. anion gap
C. estimation of glomerular filtration rate
D. fractional excretion of urea
E. split 24-hour urine for protein
Correct Answer: B Section: (none)
Explanation:
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti-GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Question 760:
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows:
With regard the workup of this man's proteinuria, what diagnostic test would you perform next?
A. serum and urine protein electrophoresis
B. kidney biopsy
C. complement levels
D. antiglomerular basement membrane (anti-GBM) antibody titer
E. glycosylated Hgb level
Correct Answer: A Section: (none)
Explanation:
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti-GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.