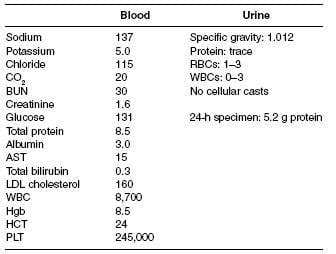
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows:
Which of the following is a typical finding in this patient's condition?
A. hypocalcemia
B. macrocytic anemia
C. elevated thyroxine levels
D. hypocomplementemia
E. hematuria
Correct Answer: A Section: (none)
Explanation:
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic
syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti-GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Question 762:
A 53-year-old White female, with a history of systemic lupus erythematosus (SLE), hypertension, and peripheral vascular disease, is admitted to the hospital for chest pain and dyspnea. Her cardiac enzymes were positive for acute MI. She subsequently undergoes a cardiac catheterization and stenting of the right coronary artery. Her postcardiac catheterization course is unremarkable, and she is discharged home 3 days later with adequate blood pressure control. Five days later, she is brought to the ER by her husband for abdominal pain and nausea. Her medications consist of aspirin, metoprolol, and prednisone. On physical examination, her blood pressure is 190/95 and her heart rate is 85 bpm. In general, she appears nauseated but is in no acute distress. Her cardiac examination reveals a regular rate and rhythm without murmur or rub. Her lung fields are clear bilaterally. The abdominal examination is positive for diffuse discomfort, without guarding or rebound, and normoactive bowel sounds; her stool is positive for occult blood. Her lower extremities have trace edema bilaterally with 2+ distal pulses; moreover, she has a reddish-blue discoloration on both her lower extremities. You retrieve her records from prior hospitalization. The patient's laboratory results are as follows:
Which of the following is the optimal therapeutic agent for this patient's pain management?
A. intravenous Demerol
B. intramuscular ketorolac
C. oral indomethacin
D. intravenous morphine sulfate
E. ibuprofen 400 mg orally three times daily as needed
Correct Answer: D Section: (none)
Explanation:
This patient has atheroembolic disease, most likely from the dislodging of arterial plaque during or after the cardiac catheterization, with subsequent kidney embolization. The findings in her history and physical examination that would suggest this are the presence of significant hypertension, abdominal pain, the redblue rash on her extremities (livedo reticularis), and eosinophilia with urinary eosinophils. Furthermore, the time course of the development of acute renal failure is suggestive of atheroembolic disease. The typical time course for contrast nephropathy is of an immediate onset, usually with subsequent recovery.
However, in patients with atheroembolic disease, the kidney failure can occur much later after the procedure. Contrast nephropathy is not associated with the laboratory abnormalities and physical examination findings seen in this case. Interstitial nephritis is unlikely, as is a lupus nephritis flare, given her classic presentation for emboli. Calculation of the fractional excretion of sodium (FeNa) is helpful in differentiating between "prerenal" causes (FeNa <1%) of acute renal failure versus intrinsic causes (FeNa >1%). A kidney ultrasound is helpful in determining the presence of urinary tract obstruction. Neither the anion gap nor calculation of glomerular filtration rate is helpful in determining if volume depletion is a possible etiology of acute renal failure. Examination of urine sediment would be helpful in determining the presence of a glomerular etiology of acute renal failure, not a prerenal etiology. Demerol and metabolites can accumulate in patients with depressed kidney function, leading to increased levels and, potentially, convulsions. NSAIDs should be avoided in patients with acute kidney failure, as these drugs are potential nephrotoxins and could prevent a recovery of kidney function. Ketorolac, indomethacin, and ibuprofen are all NSAIDs. Therefore, morphine is the best option of those given.WBC casts are suggestive of pyelonephritis. High levels of proteinuria are significant for the diagnosis of nephrotic syndrome, but not lupus nephritis specifically. Urine eosinophils are usually seen in patients with acute interstitial nephritis or atheroembolic disease. Lupus nephritis is usually associated with depressed serum complement levels. Of these tests, RBC casts are the most suggestive of glomerulonephritis.
Question 763:
A 53-year-old White female, with a history of systemic lupus erythematosus (SLE), hypertension, and peripheral vascular disease, is admitted to the hospital for chest pain and dyspnea. Her cardiac enzymes were positive for acute MI. She subsequently undergoes a cardiac catheterization and stenting of the right coronary artery. Her postcardiac catheterization course is unremarkable, and she is discharged home 3 days later with adequate blood pressure control. Five days later, she is brought to the ER by her husband for abdominal pain and nausea. Her medications consist of aspirin, metoprolol, and prednisone. On physical examination, her blood pressure is 190/95 and her heart rate is 85 bpm. In general, she appears nauseated but is in no acute distress. Her cardiac examination reveals a regular rate and rhythm without murmur or rub. Her lung fields are clear bilaterally. The abdominal examination is positive for diffuse discomfort, without guarding or rebound, and normoactive bowel sounds; her stool is positive for occult blood. Her lower extremities have trace edema bilaterally with 2+ distal pulses; moreover, she has a reddish-blue discoloration on both her lower extremities. You retrieve her records from prior hospitalization. The patient's laboratory results are as follows:
Which of the following tests is helpful in distinguishing volume depletion as a possible cause of acute renal failure?
A. kidney ultrasound
B. calculation of the fractional excretion of sodium
C. estimation of the glomerular filtration rate
D. examination of the urine sediment under microscopy
E. calculation of the anion gap
Correct Answer: B Section: (none)
Explanation:
This patient has atheroembolic disease, most likely from the dislodging of arterial plaque during or after the cardiac catheterization, with subsequent kidney embolization. The findings in her history and physical examination that would suggest this are the presence of significant hypertension, abdominal pain, the redblue rash on her extremities (livedo reticularis), and eosinophilia with urinary eosinophils. Furthermore, the time course of the development of acute renal failure is suggestive of atheroembolic disease. The typical time course for contrast nephropathy is of an immediate onset, usually with subsequent recovery. However, in patients with atheroembolic disease, the kidney failure can occur much later after the procedure. Contrast nephropathy is not associated with the laboratory abnormalities and physical examination findings seen in this case. Interstitial nephritis is unlikely, as is a lupus nephritis flare, given her classic presentation for emboli. Calculation of the fractional excretion of sodium (FeNa) is helpful in differentiating between "prerenal" causes (FeNa <1%) of acute renal failure versus intrinsic causes (FeNa >1%). A kidney ultrasound is helpful in determining the presence of urinary tract obstruction. Neither the anion gap nor calculation of glomerular filtration rate is helpful in determining if volume depletion is a possible etiology of acute renal failure. Examination of urine sediment would be helpful in determining the presence of a glomerular etiology of acute renal failure, not a prerenal etiology. Demerol and metabolites can accumulate in patients with depressed kidney function, leading to increased levels and, potentially, convulsions. NSAIDs should be avoided in patients with acute kidney failure, as these drugs are potential nephrotoxins and could prevent a recovery of kidney function. Ketorolac, indomethacin, and ibuprofen are all NSAIDs. Therefore, morphine is the best option of those given.WBC casts are suggestive of pyelonephritis. High levels of proteinuria are significant for the diagnosis of nephrotic syndrome, but not lupus nephritis specifically. Urine eosinophils are usually seen in patients with acute interstitial nephritis or atheroembolic disease. Lupus nephritis is usually associated with depressed serum complement levels. Of these tests, RBC casts are the most suggestive of glomerulonephritis.
Question 764:
A 53-year-old White female, with a history of systemic lupus erythematosus (SLE), hypertension, and peripheral vascular disease, is admitted to the hospital for chest pain and dyspnea. Her cardiac enzymes were positive for acute MI. She subsequently undergoes a cardiac catheterization and stenting of the right coronary artery. Her postcardiac catheterization course is unremarkable, and she is discharged home 3 days later with adequate blood pressure control. Five days later, she is brought to the ER by her husband for abdominal pain and nausea. Her medications consist of aspirin, metoprolol, and prednisone. On physical examination, her blood pressure is 190/95 and her heart rate is 85 bpm. In general, she appears nauseated but is in no acute distress. Her cardiac examination reveals a regular rate and rhythm without murmur or rub. Her lung fields are clear bilaterally. The abdominal examination is positive for diffuse discomfort, without guarding or rebound, and normoactive bowel sounds; her stool is positive for occult blood. Her lower extremities have trace edema bilaterally with 2+ distal pulses; moreover, she has a reddish-blue discoloration on both her lower extremities. You retrieve her records from prior hospitalization. The patient's laboratory results are as follows:
What is the most likely cause of this patient's acute renal failure?
A. contrast nephropathy from cardiac catheterization
B. acute interstitial nephritis
C. prerenal etiology from occult gastrointestinal (GI) bleeding
D. atheroembolic disease
E. lupus nephritis flare
Correct Answer: D Section: (none)
Explanation:
This patient has atheroembolic disease, most likely from the dislodging of arterial plaque during or after the cardiac catheterization, with subsequent kidney embolization. The findings in her history and physical examination that would suggest this are the presence of significant hypertension, abdominal pain, the redblue rash on her extremities (livedo reticularis), and eosinophilia with urinary eosinophils. Furthermore, the time course of the development of acute renal failure is suggestive of atheroembolic disease. The typical time course for contrast nephropathy is of an immediate onset, usually with subsequent recovery. However, in patients with atheroembolic disease, the kidney failure can occur much later after the procedure. Contrast nephropathy is not associated with the laboratory abnormalities and physical examination findings seen in this case. Interstitial nephritis is unlikely, as is a lupus nephritis flare, given her classic presentation for emboli. Calculation of the fractional excretion of sodium (FeNa) is helpful in differentiating between "prerenal" causes (FeNa <1%) of acute renal failure versus intrinsic causes (FeNa >1%). A kidney ultrasound is helpful in determining the presence of urinary tract obstruction. Neither the anion gap nor calculation of glomerular filtration rate is helpful in determining if volume depletion is a possible etiology of acute renal failure. Examination of urine sediment would be helpful in determining the presence of a glomerular etiology of acute renal failure, not a prerenal etiology. Demerol and metabolites can accumulate in patients with depressed kidney function, leading to increased levels and, potentially, convulsions. NSAIDs should be avoided in patients with acute kidney failure, as these drugs are potential nephrotoxins and could prevent a recovery of kidney function. Ketorolac, indomethacin, and ibuprofen are all NSAIDs. Therefore, morphine is the best option of those given.WBC casts are suggestive of pyelonephritis. High levels of proteinuria are significant for the diagnosis of nephrotic syndrome, but not lupus nephritis specifically. Urine eosinophils are usually seen in patients with acute interstitial nephritis or atheroembolic disease. Lupus nephritis is usually associated with depressed serum complement levels. Of these tests, RBC casts are the most suggestive of glomerulonephritis.
Question 765:
A 53-year-old Black male, with a history of hypertension, hepatitis C, and newly diagnosed nonsmall cell lung cancer, undergoes his first round of chemotherapy, which includes cisplatin. You are called to see this patient 5 days into his hospitalization for oliguria and laboratory abnormalities. Other than the chemotherapy, he is receiving lansoprazole, acetaminophen, and an infusion of D5--0.9% normal saline at 50 mL/h. On examination, his BP is 98/60 and heart rate is irregular, between 40 and 50 bpm. His physical examination shows a middle-aged male in no acute distress. His cardiac examination is unremarkable, his lungs show bibasilar crackles, and the abdominal examination is positive for a palpable spleen tip without any hepatomegaly or abdominal tenderness. He has trace bilateral ankle edema. His distal pulses are irregular. The neurologic examination was unremarkable. His laboratory (serum sample) results are as follows Which of the following would be a part of the IMMEDIATE treatment strategy in this patient?
A. atropine 1 mg IV
B. calcium chloride, given IV
C. 50 g of Kayexalate, given orally
D. 10 units of regular insulin, given subcutaneously
E. one ampule of glucagon, given IV
Correct Answer: B Section: (none)
Explanation:
The patient has tumor lysis syndrome. The destruction of malignant cells by chemotherapeutic agents will lead to the release of intracellular contents, including potassium, phosphorus, and uric acid (from nucleic acids). This can result in hyperkalemia, hyperuricemia, and hyperphosphatemia. Hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. The presence of bradycardia and irregular heart rate on physical examination are suggestive of the cardiac effects of hyperkalemia, which can lead to lifethreatening arrhythmias if not addressed. Patients with tumor lysis syndrome can develop a severe hyperuricemia. The kidneys are responsible for the excretion of uric acid. In acidic urine, the uric acid can crystallize in collecting tubules, resulting in intratubular obstruction and acute kidney failure. Calcium oxalate stones are not a part of this entity. Cisplatin can cause renal potassium and magnesium losses, which is not the case in this patient. The laboratory data suggest the release of intracellular contents (high LDH, uric acid, potassium, and phosphate) and the diagnosis of urate nephropathy as the cause of his acute kidney failure. As mentioned before, hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. Prominent U waves are found in hypokalemia, not hyperkalemia. Atrial fibrillation is not typically seen in hyperkalemia
Question 766:
A 53-year-old Black male, with a history of hypertension, hepatitis C, and newly diagnosed nonsmall cell lung cancer, undergoes his first round of chemotherapy, which includes cisplatin. You are called to see this patient 5 days into his hospitalization for oliguria and laboratory abnormalities. Other than the chemotherapy, he is receiving lansoprazole, acetaminophen, and an infusion of D5--0.9% normal saline at 50 mL/h. On examination, his BP is 98/60 and heart rate is irregular, between 40 and 50 bpm. His physical examination shows a middle-aged male in no acute distress. His cardiac examination is unremarkable, his lungs show bibasilar crackles, and the abdominal examination is positive for a palpable spleen tip without any hepatomegaly or abdominal tenderness. He has trace bilateral ankle edema. His distal pulses are irregular. The neurologic examination was unremarkable. His laboratory (serum sample) results are as follows What would be the most likely finding on this patient's ECG?
A. shortened P-R segment
B. prominent U wave
C. widened QRS complexes
D. flattened T waves
E. atrial fibrillation
Correct Answer: C Section: (none)
Explanation:
The patient has tumor lysis syndrome. The destruction of malignant cells by chemotherapeutic agents will lead to the release of intracellular contents, including potassium, phosphorus, and uric acid (from nucleic acids). This can result in hyperkalemia, hyperuricemia, and hyperphosphatemia. Hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. The presence of bradycardia and irregular heart rate on physical examination are suggestive of the cardiac effects of hyperkalemia, which can lead to lifethreatening arrhythmias if not addressed. Patients with tumor lysis syndrome can develop a severe hyperuricemia. The kidneys are responsible for the excretion of uric acid. In acidic urine, the uric acid can crystallize in collecting tubules, resulting in intratubular obstruction and acute kidney failure. Calcium oxalate stones are not a part of this entity. Cisplatin can cause renal potassium and magnesium losses, which is not the case in this patient. The laboratory data suggest the release of intracellular contents (high LDH, uric acid, potassium, and phosphate) and the diagnosis of urate nephropathy as the cause of his acute kidney failure. As mentioned before, hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. Prominent U waves are found in hypokalemia, not hyperkalemia. Atrial fibrillation is not typically seen in hyperkalemia
Question 767:
A 53-year-old Black male, with a history of hypertension, hepatitis C, and newly diagnosed nonsmall cell lung cancer, undergoes his first round of chemotherapy, which includes cisplatin. You are called to see this patient 5 days into his hospitalization for oliguria and laboratory abnormalities. Other than the chemotherapy, he is receiving lansoprazole, acetaminophen, and an infusion of D5--0.9% normal saline at 50 mL/h. On examination, his BP is 98/60 and heart rate is irregular, between 40 and 50 bpm. His physical examination shows a middle-aged male in no acute distress. His cardiac examination is unremarkable, his lungs show bibasilar crackles, and the abdominal examination is positive for a palpable spleen tip without any hepatomegaly or abdominal tenderness. He has trace bilateral ankle edema. His distal pulses are irregular. The neurologic examination was unremarkable. His laboratory (serum sample) results are as follows What is the most likely etiology of this patient's acute renal failure?
A. renal tubular deposition of uric acid
B. calcium oxalate kidney stones causing partial urinary tract obstruction
C. renal tubular injury due to cisplatin
D. ischemic acute tubular necrosis from a decreased cardiac output
E. type II cryoglobulinemia due to hepatitis C
Correct Answer: A Section: (none)
Explanation:
The patient has tumor lysis syndrome. The destruction of malignant cells by chemotherapeutic agents will lead to the release of intracellular contents, including potassium, phosphorus, and uric acid (from nucleic acids). This can result in hyperkalemia, hyperuricemia, and hyperphosphatemia. Hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. The presence of bradycardia and irregular heart rate on physical examination are suggestive of the cardiac effects of hyperkalemia, which can lead to lifethreatening arrhythmias if not addressed. Patients with tumor lysis syndrome can develop a severe hyperuricemia. The kidneys are responsible for the excretion of uric acid. In acidic urine, the uric acid can crystallize in collecting tubules, resulting in intratubular obstruction and acute kidney failure. Calcium oxalate stones are not a part of this entity. Cisplatin can cause renal potassium and magnesium losses, which is not the case in this patient. The laboratory data suggest the release of intracellular contents (high LDH, uric acid, potassium, and phosphate) and the diagnosis of urate nephropathy as the cause of his acute kidney failure. As mentioned before, hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. Prominent U waves are found in hypokalemia, not hyperkalemia. Atrial fibrillation is not typically seen in hyperkalemia
Question 768:
A 53-year-old Black male, with a history of hypertension, hepatitis C, and newly diagnosed nonsmall cell lung cancer, undergoes his first round of chemotherapy, which includes cisplatin. You are called to see this patient 5 days into his hospitalization for oliguria and laboratory abnormalities. Other than the chemotherapy, he is receiving lansoprazole, acetaminophen, and an infusion of D5--0.9% normal saline at 50 mL/h. On examination, his BP is 98/60 and heart rate is irregular, between 40 and 50 bpm. His physical examination shows a middle-aged male in no acute distress. His cardiac examination is unremarkable, his lungs show bibasilar crackles, and the abdominal examination is positive for a palpable spleen tip without any hepatomegaly or abdominal tenderness. He has trace bilateral ankle edema. His distal pulses are irregular. The neurologic examination was unremarkable. His laboratory (serum sample) results are as follows Which electrolyte/acid-base abnormality is most likely responsible for the findings on physical examination?
A. hypernatremia
B. hyperkalemia
C. metabolic acidosis
D. hyperphosphatemia
E. hyperuricemia
Correct Answer: B Section: (none)
Explanation:
The patient has tumor lysis syndrome. The destruction of malignant cells by chemotherapeutic agents will lead to the release of intracellular contents, including potassium, phosphorus, and uric acid (from nucleic acids). This can result in hyperkalemia, hyperuricemia, and hyperphosphatemia. Hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. The presence of bradycardia and irregular heart rate on physical examination are suggestive of the cardiac effects of hyperkalemia, which can lead to lifethreatening arrhythmias if not addressed. Patients with tumor lysis syndrome can develop a severe hyperuricemia. The kidneys are responsible for the excretion of uric acid. In acidic urine, the uric acid can crystallize in collecting tubules, resulting in intratubular obstruction and acute kidney failure. Calcium oxalate stones are not a part of this entity. Cisplatin can cause renal potassium and magnesium losses, which is not the case in this patient. The laboratory data suggest the release of intracellular contents (high LDH, uric acid, potassium, and phosphate) and the diagnosis of urate nephropathy as the cause of his acute kidney failure. As mentioned before, hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. Prominent U waves are found in hypokalemia, not hyperkalemia. Atrial fibrillation is not typically seen in hyperkalemia.
Question 769:
A 68-year-old White male, with a history of hypertension, an 80 pack-year history of tobacco use and emphysema, is brought into the ER because of 4 days of progressive confusion and lethargy. His wife notes that he takes amlodipine for his hypertension. He does not use over-the-counter (OTC) medications, alcohol, or drugs. Furthermore, she indicates that he has unintentionally lost approximately 30 lbs in the last 6 months. His physical examination shows that he is afebrile with a blood pressure of 142/85, heart rate of 92 (no orthostatic changes), and a room-air O2 saturation of 91%. He is 70 kg. The patient appears cachectic. He is arousable but lethargic and unable to follow any commands. His mucous membranes are moist, heart rate regular without murmurs or a S3/S4 gallop, and extremities without any edema. His pulmonary examination shows mildly diminished breath sounds in the right lower lobe with wheezing bilaterally. The patient is unable to follow commands during neurologic examination but moves all his extremities spontaneously. Laboratory results are as follows:
Blood Sodium: 109 Potassium: 3.8 Chloride: 103 CO2: 33 BUN: 17 Creatinine: 1.1 Glucose: 95 Urine osmolality: 600 Plasma osmolality: 229 White blood cell (WBC): 8000 Hgb: 15.8 Hematocrit (HCT): 45.3 Platelets: 410 Arterial blood gas: pH 7.36/pCO2 60/pO2 285 A chest x-ray (CXR) reveals a large right hilar mass.
Which of the following is the correct statement regarding the treatment of hyponatremia?
A. Desmopressin acetate (DDAVP), used in conjunction with intravenous saline, will help correct the serum sodium.
B. Correction of sodium slowly by 3 meq/day will prevent any subsequent neurologic injury.
C. Correction of serum sodium by 15 meq over 24 hours could lead to permanentneurologic injury.
D. Diuretics should be avoided in the treatment of hyponatremia.
E. Potassium should always be added to IV saline solutions when treating both hyponatremia and hypokalemia.
Correct Answer: C Section: (none)
Explanation:
The patient has hypotonic hyponatremia, which can lead to increased water shifting into the brain, resulting in cerebral edema. This patient has nothing in history or physical examination to suggest a stroke or the presence of sepsis as the etiology of his altered mental status. Central pontine myelinolysis is a potentially devastating neurologic complication that can result from the treatment of hyponatremia, not hyponatremia itself. While respiratory acidosis could potentially contribute to this patient's change in mental status, cerebral edema due to hypotonicity is the most likely etiology. The patient's laboratory studies indicate a low plasma osmolality with an inappropriately increased urine osmolality. With this degree of hypotonicity, the urine should be maximally dilute (osmolality of <100 mOsmol/kg H2O). The high urine osmolality suggests the presence of antidiuretic hormone. In psychogenic polydipsia, the urine would be maximally dilute. Choice C is unlikely since his physical examination does not suggest volume depletion; furthermore, the patient is taking a calcium channel blocker, not a diuretic, for the treatment of his hypertension. Decreased expression of renal collecting duct water channels would lead to water wasting and, thus, the development of diabetes insipidus and hypernatremia. The patient has symptomatic hypotonic hyponatremia with signs of cerebral edema.
This requires immediate attention. Choices A, C, and E are essentially hypotonic solutions which should be withheld in patients with hyponatremia. The serum sodium in this case should be increased by at least 5% for the treatment of cerebral edema. The use of 0.9% saline would require nearly 5 L of infusate to address this cerebral edema. This could lead to pulmonary edema and volume overload. The use of hypertonic saline (3% saline) is the ideal solution to use in this scenario, as the infusion of 3% saline will correct the symptoms while avoiding volume overload. As in all cases of hyponatremia management, frequent serum sodium assays are necessary in order to avoid too rapid of a correction, which could result in neurologic injury--pontine myelinolysis.
Question 770:
A 68-year-old White male, with a history of hypertension, an 80 pack-year history of tobacco use and emphysema, is brought into the ER because of 4 days of progressive confusion and lethargy. His wife notes that he takes amlodipine for his hypertension. He does not use over-the-counter (OTC) medications, alcohol, or drugs. Furthermore, she indicates that he has unintentionally lost approximately 30 lbs in the last 6 months. His physical examination shows that he is afebrile with a blood pressure of 142/85, heart rate of 92 (no orthostatic changes), and a room-air O2 saturation of 91%. He is 70 kg. The patient appears cachectic. He is arousable but lethargic and unable to follow any commands. His mucous membranes are moist, heart rate regular without murmurs or a S3/S4 gallop, and extremities without any edema. His pulmonary examination shows mildly diminished breath sounds in the right lower lobe with wheezing bilaterally. The patient is unable to follow commands during neurologic examination but moves all his extremities spontaneously. Laboratory results are as follows:
Blood Sodium: 109 Potassium: 3.8 Chloride: 103 CO2: 33 BUN: 17 Creatinine: 1.1 Glucose: 95 Urine osmolality: 600 Plasma osmolality: 229 White blood cell (WBC): 8000 Hgb: 15.8 Hematocrit (HCT): 45.3 Platelets: 410 Arterial blood gas: pH 7.36/pCO2 60/pO2 285 A chest x-ray (CXR) reveals a large right hilar mass.
Which of the following would be the optimal choice of solution to infuse in order to adequately correct this patient's hyponatremia?
A. D5W with 20 meq/L KCl at 200 mL/h
B. 0.9% saline at 125 mL/h
C. 0.45% saline at 100 mL/h
D. 3% saline at 35 mL/h
E. 0.45% saline with 30 meq/L KCl at 100 mL/h
Correct Answer: D Section: (none)
Explanation:
The patient has hypotonic hyponatremia, which can lead to increased water shifting into the brain, resulting in cerebral edema. This patient has nothing in history or physical examination to suggest a stroke or the presence of sepsis as the etiology of his altered mental status. Central pontine myelinolysis is a potentially devastating neurologic complication that can result from the treatment of hyponatremia, not hyponatremia itself. While respiratory acidosis could potentially contribute to this patient's change in mental status, cerebral edema due to hypotonicity is the most likely etiology. The patient's laboratory studies indicate a low plasma osmolality with an inappropriately increased urine osmolality. With this degree of hypotonicity, the urine should be maximally dilute (osmolality of <100 mOsmol/kg H2O). The high urine osmolality suggests the presence of antidiuretic hormone. In psychogenic polydipsia, the urine would be maximally dilute. Choice C is unlikely since his physical examination does not suggest volume depletion; furthermore, the patient is taking a calcium channel blocker, not a diuretic, for the treatment of his hypertension. Decreased expression of renal collecting duct water channels would lead to water wasting and, thus, the development of diabetes insipidus and hypernatremia. The patient has symptomatic hypotonic hyponatremia with signs of cerebral edema.
This requires immediate attention. Choices A, C, and E are essentially hypotonic solutions which should be withheld in patients with hyponatremia. The serum sodium in this case should be increased by at least 5% for the treatment of cerebral edema. The use of 0.9% saline would require nearly 5 L of infusate to address this cerebral edema. This could lead to pulmonary edema and volume overload. The use of hypertonic saline (3% saline) is the ideal solution to use in this scenario, as the infusion of 3% saline will correct the symptoms while avoiding volume overload. As in all cases of hyponatremia management, frequent serum sodium assays are necessary in order to avoid too rapid of a correction, which could result in neurologic injury--pontine myelinolysis.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.