Which of the following drugs inhibit osteoclastic activity more than osteoblastic activity and have been beneficial in osteoporosis, hypercalcemia of malignancy, and Paget disease?
A. alendronate
B. calcitonin
C. fluoride
D. parathyroid hormone
E. vitamin D
Correct Answer: A
Section: Pharmacology Alendronate is a bisphosphonate, the class of drugs that has proved most effective in the treatment and prevention of osteoporosis. This class of drug is also useful in the management of hypercalcemia and certain neoplasms. Calcitonin (choice B) has been shown to slow bone loss in postmenopausal women and to treat postoperative pancreatitis. Fluoride (choice C) is used primarily in the prevention of dental caries. Parathyroid hormone (choice D), marketed as Forteo, is currently used in the clinic to treat osteoporosis. Vitamin D (choice E) has shown benefit in increasing bone deposition in osteoporotic patients. However, choices BE do not have clinical use in the treatment of malignancy or Paget disease.
Question 202:
Which of the following responses to sympathetic nerve discharge is mediated at the effector cell by acetylcholine?
A. decreased blood flow in the skin
B. increased blood fatty acids
C. increased blood glucose
D. increased heart rate
E. increased sweating
Correct Answer: E
Section: Pharmacology Thermoregulatory sweating is mediated by muscarinic receptors and is induced by the release of acetylcholine from cholinergic sympathetic nerve fibers. Therefore, sympathetic sweating can be mimicked by administration of muscarinic agonists such as bethanechol. Choices A through D are effects mediated by alpha- (choice A) or beta adrenoreceptors (choices B, C, D).
Question 203:
Which of the following receptor types is associated with the most rapid response time?
A. G-protein-coupled receptors (e.g., muscarinic receptors)
B. ion channel receptors (e.g., nicotinic receptors)
C. Jak-STAT receptors (e.g., for cytokines)
D. steroid receptors (e.g., for corticosteroids) E. transmembrane enzyme receptors (e.g., for insulin)
Correct Answer: B
Section: Pharmacology Response times for ion channel receptors are measured in milliseconds, for G proteincoupled receptors (choice A), transmembrane enzyme receptors (choice E), and Jak-STAT receptors (choice C) in seconds to minutes, and for steroid receptors (choice D) in hours or days.
Question 204:
Which of the following drugs acts primarily on an intracellular receptor?
A. abciximab
B. dexamethasone
C. insulin
D. propranolol
E. salmeterol
Correct Answer: B
Section: Pharmacology Dexamethasone, a corticosteroid, combines with a cytoplasmic steroid receptor, enters the nucleus, and alters gene expression. The other agents listed (choices A, CE) act on membrane receptors.
Question 205:
A 22-year-old man is evaluated for repeated episodes of pulmonary infections, including a recent one that is productive of foul, purulent sputum, accompanied by shortness of breath. Past medical history is also significant for chronic sinus infections with mucopurulent discharge. Physical examination is remarkable for scattered rhonchi and rales throughout all lung fields. Imaging studies show abnormally dilated and thickened airways extending close to the pleural surface and a cardiac silhouette in the right thorax. Bronchoscopy demonstrates numerous mucopurulent plugs. Which of the following is most likely responsible for these changes?
A. abnormal neutrophilic function resulting in impaired degranulation
B. alpha-1 antiprotease deficiency (PiZZ phenotype)
C. cell membrane defect resulting in abnormally viscous glandular secretions
D. defect in ciliary motility due to the absence of dynein arms
E. hypersensitivity reaction associated with c-ANCA and granuloma formation
Correct Answer: D
Section: Pathology and Path physiology Kartagener syndrome is defined by the triad of bronchiectasis, sinusitis, and situs inversus that, in this patient, were apparent from the foul sputum, history of sinusitis, and location of the heart in the right chest. The cause of this syndrome is the lack of ciliary motility leading to poor clearing of the respiratory tract and susceptibility to infections. During embryogenesis, cilia assist with cell migration and the situs inversus is most probably the result of their lack of function. Abnormal neutrophilic function resulting in impaired degranulation (choice A) has been observed in different conditions including in HIV-infected patients but this cannot explain the situs inversus. Alpha-1 antiprotease deficiency (PiZZ phenotype) (choice B) is a cause of emphysema and liver cirrhosis, but is not associated with the findings in this patient. Cell membrane defect resulting in abnormally viscous glandular secretions (choice C) is a description of cystic fibrosis that is associated, among other things, with recurrent lung infections but not situs inversus. Hypersensitivity disease associated with c-ANCA and granuloma formation (choice E) is a description of Wegener granulomatosis which is associated with lung infections and sinusitis, but once again has no association with situs inversus.
Question 206:
A 28-year-old woman with no significant past medical history presents to her primary care physician complaining of a chronic productive cough with blood-tinged sputum, night sweats, low-grade fever, and a 15-lbs weight loss over the past 6 weeks. Chest x-ray reveals a cavitary lesion in the left upper lobe and a calcified left hilar lymph node. Biopsy of the left upper lobe mass would most likely demonstrate which of the following?
A. amorphous eosinophilic material surrounded by epithelioid cells and T-lymphocytes
B. disorganized pleomorphic and hyperchromatic cells with rare mitotic figures
C. numerous neutrophils and necrotic debris surrounded by a fibrous capsule
D. scattered macrophages interspersed with regenerating alveolar cells and sparse collagen deposition
E. sheets of small, uniform basophilic cells with large nuclei and scant cytoplasm
Correct Answer: A
Section: Pathology and Path physiology This clinical scenario describes secondary tuberculosis (TB). Upon initial exposure to the bacillus, an individual develops primary TB, where M. tuberculosis is phagocytosed by alveolar macrophages and transported to the hilar lymph nodes. As naïve macrophages are unable to kill the mycobacterium, bacteria multiply and lyse the host cell, at which time they infect other macrophages. T-cell immunity develops after a few weeks to control the initial infection. An epithelioid-cell granulomatous inflammation occurs at the site of original parenchymal infection, which, upon healing, results in scar formation, at times with late calcification that may leave a residual lesion potentially visible on chest x- ray. This parenchymal scar in association with an enlarged (and possibly calcified) hilar lymph node is known as the Ghon complex. In approximately 9095% of immunocompetent individuals, complete healing occurs. Because M. tuberculosis may persist within macrophages for many years, reactivation may occur, although the mechanisms responsible for keeping the bacilli dormant as well as those leading to reactivation are unknown. Reactivation (or, on less frequent occasions, reinfection) of TB is known as secondary TB. Typical clinical symptoms include weight loss, low-grade fever, and drenching night sweats. Reactivated TB has a predilection for the upper lung zones, presumably due to the greater availability of oxygen in this area, which enhances multiplication of the aerobic bacilli. An enhanced delayed hypersensitivity reaction results in an amplified local inflammatory response with extensive caseous necrosis. Multiple, small granulomas coalesce to form a large solid mass of fibrocaseous granulomatous inflammation known as a tuberculoma. Caseous necrosis undergoes liquefaction, and with extension of disease may erode into a bronchus, which leads to cavitation of the tuberculoma and coughing up of infectious, potentially bloody sputum. Microscopically, granulomatous inflammation is demonstrated by a central area of amorphous, eosinophilic material surrounded by epithelioid cells, frequently with Langhans-type giant cells, and an outer rim of predominantly T-lymphocytes. Disorganized pleomorphic and hyperchromatic cells with rare mitotic figures (choice B) is a generic description for lung carcinoma. Numerous neutrophils and necrotic debris surrounded by a fibrous capsule (choice C) would be suggestive of a chronic abscess, while scattered macrophages interspersed with regenerating alveolar cells and sparse collagen deposition (choice D) would occur following a necrotizing lung infection (e.g., S. aureus). Sheets of small, uniform basophilic cells with large nuclei and scant cytoplasm (choice E) is the morphological description of undifferentiated small cell (oat cell) lung carcinoma.
Question 207:
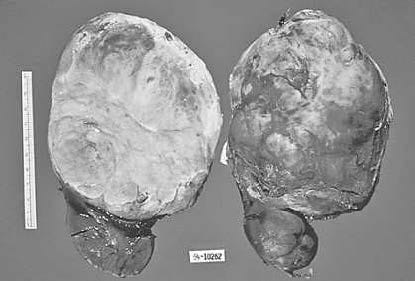
During a routine pediatric visit, you discover a large abdominal mass in a 2-year-old boy. The mass is surgically removed and is illustrated in below figure. What is the most likely diagnosis?
A. abscess
B. neuroblastoma
C. renal cell carcinoma
D. tuberculosis
E. Wilms' tumor
Correct Answer: E
Section: Pathology and Path physiology Figure shows a large tumor mass originating in the kidney. Wilms' tumor (or nephroblastoma) is the most common primary renal tumor of childhood and the second most common malignancy overall after lymphoma/ leukemia. It typically presents as a large abdominal mass discovered by a parent. An abscess (choice A) is a localized collection of pus that is not compatible with the solid mass shown here. A neuroblastoma (choice B) is most commonly primary in the adrenal and is unlikely to arise in the kidney. Renal cell carcinoma (choice C) is the most common primary renal tumor in adults, but is not expected in a child. Tuberculosis (choice D) would be identified by caseous necrosis, which has the appearance of amorphous crumbled cheese, not the solid appearance shown here.
Question 208:
A 33-year-old man comes to see you because of several episodes of hemoptysis and dyspnea during the last 2 weeks. Physical examination reveals hypertension and edema. You order some laboratory tests and the results indicate an iron-deficiency anemia, hematuria, and proteinuria with RBC casts. At this point you strongly suspect that he has which of the following diseases?
A. fibrosing alveolitis
B. Goodpasture syndrome
C. Kartagener syndrome
D. systemic lupus erythematosus
E. Wegener granulomatosis
Correct Answer: B
Section: Pathology and Path physiology Goodpasture syndrome consists of antibodies against basement membrane material, recurrent pulmonary hemorrhage, and glomerulonephritis. The pathologic changes are due to a type II hypersensitivity reaction along the basement membranes of the lung and kidney. Steroids, plasmapheresis, and immunosuppressive medicines may help in a minority of cases. Fibrosing alveolitis (choice A) is a pulmonary disorder of unknown etiology. Glomerulonephritis and pulmonary hemorrhage are not observed clinically. Kartagener syndrome (choice C) is a hereditary disease of infancy due to a defect in respiratory ciliary action. Systemic lupus erythematosus (choice D) may present with renal insufficiency. Antibodies are directed against nuclear antigens. Wegener granulomatosis (choice E) may present clinically with pulmonary hemorrhages and renal insufficiency. There are antibodies against neutrophil components, not basement membrane material.
Question 209:
A 73-year-old man is brought to his primary care physician by his wife who is concerned about her husband's progressive memory problems over the past year. She notes that he originally began forgetting to do his normal household chores, and then started routinely misplacing things around the house; he has also forgotten to close or lock doors or turn off the oven and has left the car running in the garage. He is having trouble remembering the driving routes to familiar places and names of longtime friends and acquaintances. The patient's neurological examination reveals disorientation to place and time, inability to recall three objects, and difficulty following a threestage command. Based on this information, which of the following best explains the pathogenesis of his condition?
A. cortical atrophy with neuronal cytoskeletal abnormalities and abnormal filamentous protein aggregation
B. gray matter damage to mammillary bodies and hemorrhage associated with nutritional deficiency
C. infiltrative mass of pleomorphic cells with areas of pseudopalisading, necrosis, and endothelial cell proliferation
D. injury of oligodendroglial cells with focal areas of demyelination, mononuclear infiltrate, and patchy gliosis
E. selective neuronal loss secondary to excitotoxicity associated with excessive glutamate levels
Correct Answer: A
Section: Pathology and Path physiology This patient's symptoms are very consistent with a diagnosis of AD, the most common cause of dementia in patients over 55. Over the course of this disease, patients suffer progressive impairment in higher cognitive functioning, including memory loss, spatial disorientation, language deficits, and mood and behavior changes. In end-stage AD, patients become rigid, mute, and bedridden. Definitive diagnosis of AD requires histological examination of the brain; however, with proficient clinical evaluation postmortem findings agree with clinical diagnosis in approximately 90% of cases. Grossly, brains affected by AD demonstrate cortical atrophy with widening of the sulci; changes are usually most pronounced in the frontal, temporal, and parietal lobes. With advanced disease, parenchymal atrophy results in compensatory dilation of the ventricles (hydrocephalus ex vacuo). The most severe pathology is found in the hippocampus and the nucleus basalis of Meynert of the anterior forebrain, which represent the main source of cholinergic input to the cerebral cortex. The characteristic microscopic lesions in AD are neuritic plaques and NFTs. Plaques consist of focal, spherical deposits of aggregated amyloid beta (A) fibrils surrounded by degenerating neuronal processes (dystrophic neuritis), reactive astrocytes and microglia; A plays a major role in the pathogenesis of AD. NFTs represent twisted bundles of filaments within neuronal cell bodies that extend into dendrites. Their chief constituent is a hyperphosphorylated tau protein, an axonal microtubuleassociated protein important for proper assembly and stability of microtubules, which are involved in the transport of essential molecules through the neuron. NFTs are also seen in neurodegenerative diseases other than AD. They are well demonstrated with silver stain and particularly affect pyramidal neurons (e.g., frontal cortex, hippocampus, amygdala) where they often have an elongated, flame-shaped appearance. Choice B refers to injury caused by thiamine deficiency in alcoholism; choice C describes the morphological appearance of a glioblastoma; choice D reflects changes seen in multiple sclerosis, and choice E describes biochemical changes that occur in cerebral ischemia.
Question 210:
A 52-year-old woman has experienced personality change and headaches over the past 3 months and is now developing a right hemiparesis. CT scan shows a mass in the left temporal lobe. Her condition deteriorates rapidly and she dies 7 months later. At autopsy, a large, hemorrhagic, necrotic tumor is identified in the left temporal lobe with extension to the right hemisphere. Microscopically there are highly pleomorphic cells with frequent mitoses. Serpentine areas of necrosis can be seen surrounded by masses of tumor cells. Which of the following is the most likely diagnosis?
A. ependymoma
B. glioblastoma multiforme
C. medulloblastoma
D. meningioma E. oligodendroglioma
Correct Answer: B
Section: Pathology and Path physiology Glioblastoma multiforme is the most malignant astrocytoma and is also the most common intracranial primary neoplasm. It is typically a large tumor with areas of necrosis and hemorrhage and extends to the contralateral side of the brain (butterfly tumor). Microscopically the tumor is very pleomorphic with giant cells, palisading necrosis, and endothelial proliferation. The prognosis is universally poor. Ependymoma (choice A) is somewhat more common in children and originates from the ependymal cells lining the ventricles and central canal of the spinal cord. It is a slowgrowing tumor but has the ability to seed via the cerebrospinal fluid. Medulloblastoma (choice C) is principally a highly malignant tumor of childhood that originates in the cerebellum and has the well-known ability to metastasize via the cerebrospinal fluid. Meningioma (choice D) is a benign tumor arising from the arachnoid cap cells. However, it may involve the dura and calvaria making complete removal difficult. The tumor is only considered malignant if it grows into the underlying brain. Oligodendroglioma (choice E) occurs in adults and typically arises from the white matter of the cerebrum. Most of these tumors have areas of calcification which may be seen on x-ray. Many of these tumors are mixed tumors showing areas of astrocytoma.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.