A 47-year-old man has had a cough that produces yellowish sputum for the past week. He is found to have a total WBC count of 16,300 per L with a differential count of 75% segmented neutrophils, 11% band neutrophils, 9% lymphocytes, 4% monocytes, and 1% eosinophils. His temperature is 100°F and chest x-ray reveals a lesion in the right lower lobe that has a central cavity and an air-fluid level. Which of the following is the most likely diagnosis?
A. bronchogenic carcinoma
B. interstitial pneumonia
C. lobar pneumonia
D. pulmonary abscess
E. pulmonary tuberculosis
Correct Answer: D
Section: Pathology and Path physiology The productive cough and leukocytosis with a high percentage of neutrophils and bands indicates that this is a bacterial infection and, of the choices given, is most likely an abscess. Bronchogenic carcinoma (choice A) can obstruct an airway and produce infection, but there is no evidence presented to support this. Interstitial pneumonia (choice B) is typically caused by Mycoplasma or viruses and produces a mononuclear response rather than a neutrophilic response; the cough is usually nonproductive. Lobar pneumonia (choice C) fills the affected lobe with exudate, but does not typically result in necrosis or abscess formation. Pulmonary tuberculosis (choice E) can produce a cavitary lesion, typically at the apices, but also is marked by a mononuclear response.
Question 232:
An overweight, 46-year-old man has complained of heartburn for the past 2 years. A biopsy of his lower esophagus is displayed in below figure. Which of the following is the most likely diagnosis?
A. Barrett esophagitis
B. Candida esophagitis
C. granulomatous esophagitis
D. PlummerVinson syndrome
E. viral esophagitis
Correct Answer: A
Section: Pathology and Path physiology Barrett esophagitis is a metaplastic alteration of the lower esophagus in response to chronic acid reflux. Figure displays the specialized type of Barrett esophagitis, complete with numerous goblet mucous cells. Candida esophagitis (choice B) does not contain glandular epithelium. Squamous epithelium, yeast, and pseudohyphae are expected instead. Granulomatous esophagitis (choice C) and viral esophagitis (choice E) are not characterized by metaplastic glandular epithelium. Giant cells or inclusion bodies may be seen, depending on the etiology. Plummer-Vinson syndrome (choice D) describes the formation of a lumenal web in the upper third of the esophagus. Microanatomy displays squamous epithelium, not metaplastic glandular epithelium.
Question 233:
A 46-year-old obese woman has had symptoms of vulvovaginitis for the past 9 months that is found to be caused by Candida. Laboratory tests reveal proteinuria and glucosuria, and increased serum glucose, BUN and creatinine. If a renal biopsy were performed, which of the following would be the most likely light and electron microscopic findings, respectively, in the glomeruli?
A. hypercellularity with thickened basement membranes (GBM); duplication of GBM
B. hypercellularity with PMNs; subepithelial deposits
C. normocellularity with thickened GBM; subepithelial deposits
D. normal morphology; loss of epithelial foot processes
E. thickened GBM; no deposits
Correct Answer: E
Section: Pathology and Path physiology An obese woman presenting with chronic candidal vulvovaginitis should certainly be suspected of having diabetes, and the laboratory results confirm this diagnosis. A renal biopsy of this patient would be expected to show glomerular basement membrane thickening and focal and diffuse glomerulosclerosis by light microscopy, but electron microscopy would not show any electron-dense deposits since antigen-antibody complexes are not formed in diabetes. Hypercellular glomeruli with thickened and duplicated basement membranes (tram tracks; train tracks) (choice A) is found in membranoproliferative glomerulonephritis type
1. Hypercellular glomeruli with PMNs and subepithelial deposits (humps) (choice B) are an indication for postinfectious (poststreptococcal) glomerulonephritis. Normocellular glomeruli with thickened basement membranes and subepithelial deposits (spikes) (choice C) are found in membranous glomerulopathy. Normal morphology by light microscopy with loss of epithelial foot processes by electron microscopy is a classic finding of nil disease.
Question 234:
A 21-year-old previously healthy man had a headache, malaise, and low-grade fever for the past 4 days. He was brought to the emergency room this morning after he started behaving in an unusual manner and experienced difficulty in speaking. While he was being transported, he suffered a generalized seizure. Physical examination showed a fever of 103°F and to tal disorientation. Deep tendon reflexes were exaggerated and the plantar response was bilaterally extensor. He had mild neck stiffness and the optic fundi showed early papilledema. Alumbar puncture produced clear CSF under an opening pressure of 300 mm O. Protein was 160 mg/dL, glucose 66 mg/dL (blood glucose 90
mg/dL), and there were 32 mononuclear cells/L. No PMNs were present. Which of the following is the most likely cause of this man's condition?
A. glioblastoma multiforme
B. herpetic meningoencephalitis
C. meningioma
D. meningococcal meningitis
E. spontaneous cerebral hemorrhage
F. subarachnoid hemorrhage
Correct Answer: B
Section: Pathology and Path physiology The presence of neck stiffness, the increase in the amount of protein, and the number of cells in the CSF confirm the presence of meningitis. However, the unusual behavior, disorientation, seizure, speech disorder, and abnormal reflexes represent involvement of various parts of the cerebral cortex. Thus this is an acute inflammation of the meninges and brain or a meningoencephalitis. This also accounts for the very high CSF pressure since there is brain edema in addition to the meningitis. The somewhat more prolonged course and the presence of mononuclear cells in the CSF are evidence for viral etiology making herpes the best choice of those listed and eliminating meningococcal meningitis (choice D) which elicits PMNs in the CSF and does not produce encephalitis. Tumors (choices Aand C) and hemorrhage (choices E and F) would not give this clinical presentation or CSF results.
Question 235:
A 71-year-old man was diagnosed with prostate cancer approximately 1 year ago. At that time he weighed 182 lbs (with a height of 75 in). He has progressively lost weight since then and is now found to weigh 148 lbs. Although he reports a moderate loss of appetite, it does not correlate with his total weight loss. Which of the following mediators is most likely contributing to this patient's decrease in weight?
A. C-reactive protein
B. vomplement 3a protein
C. interleukin-2
D. parathyroid hormone-related protein
E. tumor necrosis factor
Correct Answer: E
Section: Pathology and Path physiology Progressive weight loss, anorexia, and weakness comprise the wasting syndrome known as cachexia that is often associated with cancer. Although patients report anorexia and abnormalities in taste, the reduction in caloric intake does not sufficiently explain the often profound degree of wasting. While the mechanism is poorly understood, cancer frequently causes an increased metabolic rate that is postulated to occur as a result of cytokine production by both the tumor and the host response to the umor. Avariety of cytokines may function synergistically to cause cachexia; however, experimental animal studies suggest that tumor necrosis factor is the major contributor. C-reactive protein and complement 3a protein (choices Aand B) both act as opsonins in acute inflammation, while interleukin-2 (choice D) is an important growth factor for the proliferation of T-lymphocytes. Parathyroid hormonerelated protein (choice E) production is responsible for causing the hypercalcemia paraneoplastic syndrome associated with certain malignancies, most notably carcinomas of the lung and kidney.
Question 236:
A 17-year-old boy presented to his orthopedist complaining of progressive knee pain for 3 months. Physical examination revealed a swollen, warm, and tender right knee. Serum alkaline phosphatase levels were increased. Right knee x-ray revealed a lytic lesion in the metaphyseal area of the knee extending into the proximal diaphysis, and elevation of the periosteum with new bone production. Microscopically, biopsy demonstrated haphazard osteoid formation, pleomorphic cells with hyperchromatic nuclei, and tumor giant cells. Based on this information, what is the most likely diagnosis?
A. chondrosarcoma
B. Ewing sarcoma
C. giant cell tumor
D. malignant fibrous histiocytoma
E. osteosarcoma
Correct Answer: E
Section: Pathology and Path physiology In a 17-year-old boy, the anatomical location and the x-ray findings are very typical of osteosarcoma. In this case, the tumor has broken through the cortex, elevated the periosteum with reactive periosteal bone formation (the characteristic triangular shadow seen on x-ray is known radiographically as Codman triangle). The microscopic findings of pleomorphic cells with hyperchromatic nuclei, tumor giant cells, and bone formation confirm the diagnosis. Chondrosarcomas (choice A) most typically occur in the age range of 4060 with the most common locations being the pelvic girdle, ribs, shoulder girdle, and to a lesser extent the long bones, vertebrae, and sternum. Microscopically, the lower grade tumors will show chondroid differentiation, whereas a grade 3 tumor may appear as a spindle cell tumor with little chondroid differentiation. Ewing sarcomas (choice B) occur in children and young adults and usually originate in long bones, ribs, pelvis, and vertebrae. Microscopically one sees small, uniform, oval to round cells with hyperchromatic nuclei and little cytoplasm, which may appear clear due to glycogen abundance. Giant cell tumors (choice C) usually occur in the age range of 2040 most commonly originating in distal femur, proximal tibia, distal radius, and proximal humerus, but virtually any bone may be affected. These are usually benign tumors that can, however, be locally aggressive; roughly 410% do metastasize and these must be considered as malignant. Not surprisingly, the microscopic appearance is marked by the presence of many giant cells that have an osteoclast-like, syncytial appearance. Malignant fibrous histiocytomas (choice D) are fibroblastic, collagen-producing bone tumors that may also arise from soft tissues; indeed, they are the most common type of soft tissue sarcoma. They occur more frequently in the middle-aged and elderly but have been reported at all ages. Microscopically, lesions reveal spindle cells arranged in a whorled pattern with variable amounts of collagen deposition; also present may be large, plump cells (resembling histiocytes), tumor giant cells, many mitoses, and a chronic inflammatory infiltrate.
Question 237:
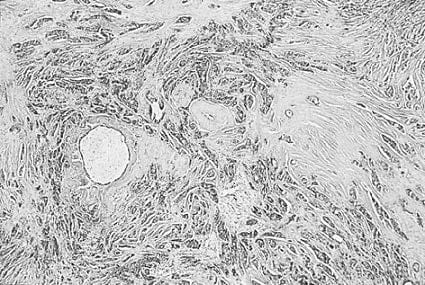
A 53-year-old woman recently noticed a firm, 2-cm nodule in her right breast during monthly self-examination. The histology of her breast biopsy tissue is displayed in below figure. Which of the following is an adverse prognostic indicator that may be seen with this disorder?
A. estrogen receptor positive
B. low S phase
C. overexpression of Her2/neu oncogene
D. progesterone receptor positive
E. well-differentiated histology, grade I of III
Correct Answer: C
Section: Pathology and Path physiology Overexpression of NEU oncogene in invasive breast carcinoma (shown in figure) is an adverse prognostic indicator. Breast cancers that are estrogen-receptor positive (choice A), have a low S phase (choice B), are progesterone-receptor positive (choice D), and are well differentiated (choice E), considered to have more favorable prognostic implications. Size of the primary breast carcinoma and the status of the axillary lymph nodes are also major factors that influence the prognosis of invasive ductal breast adenocarcinoma.
Question 238:
A 5-year-old girl has had numerous childhood fractures. She is also found to have blue sclera, hearing abnormalities, and misshapen teeth. Which of the following is the most likely cause of these findings?
A. abnormal intestinal receptors for calcium
B. an inability to metabolize vitamin D
C. inadequate mineralization of bone matrix
D. renal inability to conserve phosphorous
E. synthesis of abnormal type I collagen
Correct Answer: E
Section: Pathology and Path physiology Osteogenesis imperfecta type I, is a genetic disorder characterized by synthesis of an abnormal type I collagen. Frequent childhood fractures, blue sclera, poor hearing, and misshapen teeth may all occur clinically because of the abnormal collagen synthesis. Abnormal intestinal receptors for calcium (choice A), inability to metabolize vitamin D (choice B), inadequate mineralization of bone matrix (choice C), and renal inability to conserve phosphorous (choice D) are not the primary pathologic alterations responsible for this disorder.
Question 239:
A 47-year-old woman has a 3-month history of fatigue and pruritus. A percutaneous liver biopsy reveals a nonsuppurative, granulomatous distention of medium-sized intrahepatic bile ducts. What is the most common etiology of this disorder?
A. acquired vascular abnormality
B. alcohol abuse
C. autoimmune disease
D. parasitic infection
E. viral infection
Correct Answer: C
Section: Pathology and Path physiology Primary biliary cirrhosis is an autoimmune disorder. Autoantibodies against mitochondria are usually present. Hyperbilirubinemia, steatorrhea, portal hypertension, and osteomalacia may be seen in the later stages of the disease. Vascular abnormalities (choice A), alcohol abuse (choice B), parasitic infections (choice D), and viral infections (choice E) all may mimic the clinical picture of primary biliary cirrhosis. They are not, however, the usual etiologic agents.
Question 240:
The prevalence for disease X is 1%. Anew laboratory test is positive in 99% of the patients with disease X, but half of the total of positive test results obtained correspond to patients without disease X. Based on this information, the test would be classified as which of the following?
A. sensitive and nonspecific
B. sensitive and specific
C. nonsensitive and nonspecific
D. nonsensitive and specific
Correct Answer: B
Section: Pathology and Path physiology Let us take a population of 100,000 individuals. Since the prevalence of disease X is 1%, 1000 individuals have disease X and 99,000 are disease-free. The test is positive in 99% of individuals with the disease (i.e., of the 1000 with disease, there are 990 true positives and 10 false negatives), thus the test is clearly sensitive. However, half of all positive test results are occurring in disease-free individuals. If 990 individuals with disease had a positive test result (true positives), then there must also be 990 disease-free individuals who had a positive test result. It was stated above that 99,000 are disease-free, so of these 990 have a positive test result (false positives) and the remainder (99,000 990 = 98,010) must have a negative test result (true negatives). Specificity may be defined as the percentage of individuals in a disease-free population who have a negative test result. This is mathematically equivalent to (true negatives)/(true negatives + false positives) = (98,010)/(98,010 + 990) = 98,010/99,000 = 99%. Thus the test is both sensitive and specific, and the other answers (choices A, C, D, and E) are incorrect.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.