On a routine, employment-related chest x-ray, a 26-year-old woman is found to have a solitary rib lesion appearing as a well-demarcated, radiolucent area with a ground glass appearance and cortical thinning. When questioned, the patient states that she has never experienced any pain and does not recall ever sustaining trauma to the area. Which of the following is the most likely diagnosis?
A. chondrosarcoma
B. Ewing sarcoma
C. fibrous dysplasia
D. osteogenesis imperfect
E. osteomalacia
Correct Answer: C
Section: Pathology and Path physiology This woman's findings are consistent with a diagnosis of monostotic fibrous dysplasia (FD), variably considered to be either a benign tumor or a developmental disorder in which an abnormal proliferation of mesenchymal cells replaces normal cancellous bone with immature woven bone and fibrous tissue. In 70% of cases, a single bone is affected (monostotic FD), most frequently involving the ribs, long bones, or jawbones. Patients tend to be asymptomatic and are typically diagnosed between 2030 years of age by incidental radiograph findings (as described). Multiple bone involvement occurs in 30% of cases (polyostotic FD), often affecting shoulder and pelvic girdles and craniofacial bones. These patients tend to be younger (<10) and have a more severe course, often with pain, recurrent pathological fractures, and permanent skeletal deformity. Chondrosarcoma (choice A) has a peak incidence in the fourth to sixth decades and typically involves the flat bones of the pelvic and shoulder girdles. The histological classification of these tumors is complex. The majority of the tumors (~75%) fall into the "conventional" hyaline/ myxoid category; however, some of the minority classifications such as "mesenchymal" and "clear cell" may occur in much younger individuals. Most patients with Ewing sarcoma (choice B) are 1020 years of age. Although the femur and pelvic flat bones are common sites, similar to fibrous dysplasia, these tumors present as painful enlarging masses, which frequently are warm, swollen, and tender on examination. The x-ray appearance is also quite different, demonstrating an irregular destructive lesion extending into the surrounding soft tissues and a periosteal reaction layered in an "onion-peel" fashion. Osteogenesis imperfecta (choice D) results from a deficiency in the synthesis of type I collagen. The result is a patient with very brittle bones who manifests numerous fractures during childhood. Osteomalacia (choice E) arises from a deficiency of vitamin D (comparable to rickets in children), causing inadequate mineralization and excessive production of bone matrix (osteoid) that results in deformities of weightbearing bones. There are no focal lesions as seen in this patient.
Question 262:
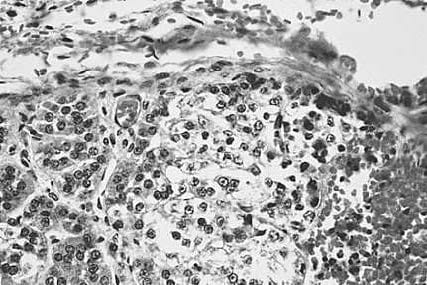
A 3-day-old girl develops numerous skin lesions followed soon thereafter by severe encephalitis. Despite extensive treatment, she dies a few days later. An autopsy examination reveals that the infant has a systemic infection involving all major organs. The photomicrograph in below figure is taken from a section of adrenal gland. Which of the following is the most likely infectious agent?
A. cytomegalovirus
B. herpes
C. rubella
D. syphilis
E. Toxoplasma
Correct Answer: B
Section: Pathology and Path physiology Figure shows areas of necrosis and cell nuclei containing Cowdry A inclusions, indicating that this is a disseminated herpes infection acquired during passage through the birth canal. Cytomegalovirus (choice A), rubella (choice C), syphilis (choice D), and Toxoplasma (choice E) are the other members of the TORCHS complex, but are typically acquired transplacentally. Cytomegalovirus (choice A) has Cowdry A nuclear inclusions but, in addition, has multiple cytoplasmic inclusions and greatly increased cell size. The other agents do not generate Cowdry A inclusions.
Question 263:
A 71-year-old man presents to his primary care physician for a check-up accompanied by his wife, who reports that she had to "push him out of the door" to go to see a doctor as his last physical examination was almost 8 years ago. He states that he has been feeling well other than having some lower back pain. Physical examination reveals a firm, nodular prostate. On further questioning, the patient states that he has not noticed any change in urination. Laboratory studies reveal a mildly elevated serum prostate-specific antigen level and a serum alkaline phosphatase level almost three times normal. These findings are most consistent with which of the following?
A. acute prostatitis
B. benign prostatic hyperplasia
C. chronic prostatitis
D. local invasion of the prostate by bladder carcinoma
E. metastatic prostate carcinoma
Correct Answer: E
Section: Pathology and Path physiology Serum prostate-specific antigen can be elevated in both benign prostatic hyperplasia and prostatic carcinoma (it is worth noting that both can also be within the reference range). However, this patient has a firm, nodular prostate with no urinary changes making carcinoma the more likely of the two. The additional finding of high levels of alkaline phosphatase is compatible with osteoblastic metastases. These findings taken together make metastatic prostate carcinoma the most likely of the choices given. Prostate-specific antigen can be elevated in acute prostatitis (choice A), benign prostatic hyperplasia (choice B), and chronic prostatitis (choice C), but none of these conditions, or local invasion of bladder carcinoma (choice D) would be expected to produce the increase in alkaline phosphatase that is seen in this case.
Question 264:
A 34-year-old woman who has been taking oral contraceptives for many years presents with acute abdominal pain and fullness. Paracentesis harvests 200 mL of bloody fluid. Imaging studies show a 6- cm mass in the liver that is subsequently resected. Histological examination of this specimen would most likely reveal this to be which of the following?
A. angiosarcoma
B. cholangiosarcoma
C. focal nodular hyperplasia
D. hepatocellular carcinoma
E. liver cell adenoma
Correct Answer: E
Section: Pathology and Path physiology Liver cell adenomas may occur after several years of taking oral contraceptives but the actual mechanism of tumor formation is unknown. The clinical presentation is often acute abdominal pain due to necrosis of the tumor and hemorrhage. Given the patient's history, liver cell adenoma is by far the most likely choice. Angiosarcomas of the liver (choice A) are very rare tumors associated with exposure to vinyl chloride (used in the manufacture of the plastic polyvinyl chloride). Cholangiosarcomas (choice B) are rare tumors that arise in the intrahepatic bile ducts. However, they are more common in the Far East, where there is an association with the liver fluke, Clonorchis sinensis. Focal nodular hyperplasia (choice C) is a tumor-like lesion that occurs more frequently in women. It has a weak association with oral contraceptive use. On cut section, it typically has a central stellate scar. It is usually asymptomatic and is only resected in the symptomatic patient. Hepatocellular carcinoma (choice D) in the United States usually arises in a background of cirrhosis due either to alcoholism or HBV infection. However, worldwide, hepatitis B is the major etiologic factor and up to 50% of patients with hepatocellular carcinoma may be noncirrhotic.
Question 265:
Alaboratory test for a newly discovered infectious disease is found to have a sensitivity of 90% and a specificity of 90%. The disease has a prevalence of 1%. The test is run on one of your patients and yields a negative result. What is the probability (to the nearest whole number) of this result being a true negative rather than a false-negative result (what is the predictive value negative)?
A. 1%
B. 10%
C. 50%
D. 90%
E. 100%
Correct Answer: E
Section: Pathology and Path physiology In a population of 100,000, 1000 people will have the disease and 99,000 will be disease free (the prevalence of the disease equals 1%). The sensitivity equals 90%, which indicates that in a population of people with the disease, 90% will have a positive test result (true positives) and 10% will have a negative test result (false negatives). The specificity also equals 90%, which indicates that in a population of people without the disease, 90% will have a negative test result (true negatives) and 10% will have a positive test result (false positives). Thus, looking at the negative test results, there were 100 false negatives (10% of the 1000 people with the disease) and 89,100 true negatives (90% of the 99,000 people without the disease). Therefore the chances of the test result being a true negative = (true negatives)/(true negatives + false negatives) = (89,100)/(89,100 + 100) = 99.9% (= 100% to the nearest whole number). Mathematically, 1% (choice A), 10% (choice B), 50% (choice C), and 90% (choice D) can be eliminated.
Question 266:
Five weeks after returning from visiting relatives in New England, a 22-year-old man develops severe headaches, fever, chills, fatigue, and multiples skin lesions. During the physical examination, the skin lesions are noted to be slightly raised and erythematous but are nontender. He states that a similar single lesion appeared on his thigh just before his return, but he was otherwise asymptomatic. Based upon this information, the most likely causative agent is which of the following?
A. Borrelia burgdorferi
B. Francisella tularensis
C. Rickettsia rickettsii
D. Toxoplasma gondii
E. Yersinia pestis
Correct Answer: A
Section: Pathology and Path physiology Lyme disease (caused by the spirochete B. burgdorferi) occurs worldwide but in the United States is found principally in northeastern and some mid-western states. It is transmitted by the Ixodes tick and the site of its bite is usually indicated by an expanding erythematous lesion with central clearing (erythema chronicum migrans (stage 1), which corresponds to the lesion the patient found just prior to his return home. Days or weeks following this stage, the organisms spread hematogenously and may cause secondary skin lesions, fever, chills, fatigue, severe headaches, arthralgias, and cardiac arrhythmias as well as many other findings (stage 2). It was at this point that the patient presented to is physician. Without treatment, many months later patients may enter stage 3 and develop more severe complications, including frank arthritis and encephalopathy. Tularemia is a zoonosis caused by F. tularensis (choice B); transmission occurs from contact with wild animals or biting insects. It is common in the southern Midwestern region. Infection typically results in an ulcerative lesion at the inoculation site and regional lymphadenopathy. R. rickettsii (choice C) causes Rocky Mountain spotted fever, the most severe of the rickettsial diseases. Intracellular infection of systemic and pulmonary endothelial cells via tick or insect vector causes a macular rash, appearing first on the wrists and ankles with subsequent spread to the full extremity and the trunk. Typically by 1 week lesions become hemorrhagic and form petechiae. Extensive microcirculatory infection may cause significant multisystemic effects, causing mortality in 35% of cases. Infection with the parasite
T. gondii (choice D) is most often associated with immunocompromised patients; transmission typically occurs from ingestion of soil contaminated with cysts shed in cat feces or from undercooked meat. Common manifestations include cervical lymphadenopathy in immunocompetent individuals and CNS involvement in the immunocompromised. Y. pestis (choice E) is the bacterium responsible for causing plague, a zoonotic disease carried by rats and wild rodents; it is transmitted to humans by bites from infected fleas. There are three forms of plague--bubonic, septicemic, and pneumonic. Bubonic is the most common, and is associated with a characteristic lymphadenopathy of rapid onset in which enlarging lymph nodes (buboes) become progressively painful and tender, often surrounded by considerable edema.
Question 267:
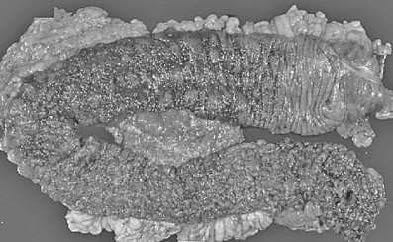
A 28-year-old man has a long history of intermittent bloody diarrhea. The colon is surgically removed and displayed in below figure. The most likely diagnosis is which of the following?
A. amebic colitis
B. collagenous colitis
C. gangrenous colitis
D. pseudomembranous colitis
E. ulcerative colitis
Correct Answer: E
Section: Pathology and Path physiology The colon segment in figure demonstrates ulcerative colitis. The disease is limited to the colon and preferentially involves in continuity the rectum, sigmoid, and descending colon. The affected colon demonstrates a red, granular mucosa with occasional pseudopolyp formation. Deep fissures, skip lesions with alternating areas of diseased and normal colon, and strictures do not typically occur. Amebic colitis (choice A) is usually limited to the right colon and displays multiple, scattered, separate ulcerations. In collagenous colitis (choice B), the colon appears grossly normal. Gangrenous colitis (choice C) has an acute clinical course. Grossly, the colon demonstrates a transmural area of blackened, thinned tissue. Pseudomembranous colitis (choice D) is usually an acute colitis occurring after antibiotic therapy. White, custard-like debris that partially coats the mucosal surface is the characteristic gross observation of pseudomembranous colitis.
Question 268:
A 15-month-old baby girl is brought to the emergency room by her parents for a 1-week history of malaise, poor feeding, mild fever, and diarrhea. Physical examination is unremarkable. This is the sixth such occasion for which the parents have brought their daughter to a physician. Past visits have revealed repeated infections, including Candida, cytomegalovirus, and M. avium-intracellulare. A complete blood count (CBC) is remarkable only for a low total lymphocyte count. Immunoglobulin levels are normal. Alymph node biopsy is remarkable for paracortical cell depletion, but is otherwise normal. Which of the following is the most likely diagnosis?
A. Bruton congenital agammaglobulinemia
B. chronic granulomatous disease of childhood
C. severe combined immunodeficiency disease
D. thymic hypoplasia
E. Wiskott-Aldrich syndrome
Correct Answer: D
Section: Pathology and Path physiology In thymic hypoplasia, the congenital developmental failure of the thymus leads to a lack of T- lymphocytes in the blood as well as in appropriate areas of lymph nodes (paracortical area). Deficient T-cell immunity will thus lead to severe, recurrent viral, mycobacterial, fungal, or protozoal infections during infancy. Thymic hypoplasia is best described in association with DiGeorge syndrome, in which defective embryological development of the third and fourth pharyngeal pouches results in developmental failure of thymus and parathyroid formation, congenital heart defects, and severe hypocalcemia, secondary to hyperparathyroidism. An associated, but less well-defined, entity is Nezelof syndrome, in which there is hypoplasia of the thymus, retention of normal parathyroid function, and possible varying degrees of humoral immunodeficiency. Bruton congenital agammaglobulinemia (choice A) is an Xlinked recessive disorder characterized by the failure of B-cell precursors to differentiate into mature B-lymphocytes, which are absent in the peripheral blood, lymph nodes, tonsils, and spleen. Serum immunoglobulin levels are decreased; however, the thymus and Tlymphocyte development are normal and cell-mediated immunity is intact. Chronic granulomatous disease of childhood (choice B) refers to a group of X-linked or autosomal recessive disorders characterized by different enzyme deficiencies of neutrophils and macrophages that lead to inhibition of hydrogen peroxide formation. Although still capable of bacterial phagocytosis, neutrophils and macrophages cannot kill bacteria, particularly the catalase-positive species such as Staphylococcus, Serratia, and Salmonella, which destroy their own endogenous hydrogen peroxide by virtue of catalase production. The disease occurs chiefly in males who present with recurrent bacterial infections of the skin, lymph nodes, lungs, and bones; widespread abscesses and granulomas are present. Severe combined immunodeficiency disease (choice C) is one of the most dramatic forms of congenital immunodeficiency in which a defect of lymphoid stem cells leads to failure of development of both Band T-lymphocytes. Although probably an embodiment of several different inherited diseases, most patients with severe combined immunodeficiency have the autosomal recessive form, and greater than half of these lack the enzyme adenosine deaminase, resulting in the accumulation of lymphotoxic metabolites. Failure of both cellular and humoral immunity causes a variety of severe viral, bacterial, fungal, and protozoal infections early in life, with death usually occurring within the first year. Wiskott-Aldrich syndrome (choice E) is an X-linked recessive disease characterized by thrombocytopenia, eczema, and immunodeficiency; both cellular and humoral immunity is impaired. Progressive T-cell deficiency occurs despite a morphologically normal thymus, and serum IgM levels are low, although IgG levels are usually normal. Recurrent bacterial, viral, and fungal infections occur, particularly with S. pneumonia and Haemophilus influenzae as these organisms have polysaccharide antigens that mainly elicit IgM antibody response. Thrombocytopenia may be severe and approximately one-third of patients die from hemorrhage. Patients are prone to developing lymphoma.
Question 269:
A 6-year-old child has a long history of a hereditary bleeding disorder characterized by spontaneous nontraumatic hemorrhages into joint spaces, skeletal muscle, and mucous membranes. Laboratory studies reveal a normal prothrombin time, elevated partial thromboplastin time, very low factor VIII, normal factor X, normal factor XI, and normal platelet aggregation studies with ristocetin. Which of the following is the most likely diagnosis?
A. Christmas disease
B. hemophilia A
C. hemophilia B
D. Rosenthal syndrome
E. von Willebrand disease
Correct Answer: B
Section: Pathology and Path physiology Hemophilia A is a genetic disorder characterized by very low levels of factor VIII, elevated partial thromboplastin time, normal prothrombin time, normal platelet aggregation with ristocetin, and spontaneous hemorrhages into joints, soft tissues, and mucosal surfaces. Christmas disease (choice A) is an alternative term for hemophilia B. Hemophilia B (choice C) is a hereditary coagulopathy due to a very low level of factor IX. Rosenthal syndrome (choice D) defines a deficiency of factor XI. von Willebrand disease (choice E) is characterized by a mild hereditary bleeding diathesis and abnormal platelet aggregation with ristocetin.
Question 270:
A 75-year-old woman, a life-long smoker with Type II diabetes, dies secondary to complications of alcoholic cirrhosis. At autopsy, a hard, infiltrative mass is observed in the head of the pancreas. Microscopic examination of the body and tail of the pancreas demonstrates acinar loss with marked fibrosis, duct dilation, some lymphocytic infiltration, and sparing of islets. Based upon the information given, which of the following would most likely represent the microscopic appearance of the pancreatic mass?
A. deposition of an acellular, eosinophilic material between parenchymal cells
B. diffuse interstitial fibrosis with intraand extracellular golden-brown pigment
C. moderately differentiated, mucussecreting cells in a dense, fibrotic stroma
D. necrosis of pancreatic parenchyma and adjacent fat with a neutrophil infiltrate E. plugging of ducts, atrophy of exocrine glands, and fibrosis
Correct Answer: C
Section: Pathology and Path physiology Little is known about the etiology of pancreatic adenocarcinoma although smoking, chronic pancreatitis, and diabetes mellitus (especially in women) have been associated with an increased risk for the disease. The microscopic description for the body and tail of the pancreas is consistent with chronic pancreatitis, thus, this woman had all three of these risk factors. The microscopic appearance of ductal pancreatic adenocarcinoma most usually (~70%) demonstrates moderately to well-differentiated cells producing mucus and surrounded by a dense fibrotic stroma. Deposition of an acellular, eosinophilic material (choice A) is a description of amyloidosis. Diffuse interstitial fibrosis with intra- and extracellular golden-brown pigment (choice B) describes hemochromatosis. Necrosis of pancreatic parenchyma and adjacent fat with inflammation (choice D) would be seen in acute pancreatitis. Plugging of ducts, atrophy of exocrine glands and fibrosis (choice E) may be seen in cystic fibrosis. In addition, choices A, B, D, and E would not be expected to be associated with a focal mass.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.