A 74-year-old man dies after a 4-day hospital course with a clinical diagnosis of adult respiratory distress syndrome. At autopsy a pathologic diagnosis of diffuse alveolar damage is rendered. Which of the following microscopic findings of the lung tissue is most expected at autopsy?
A. alveolar hyaline membrane formation
B. eosinophilic inflammatory infiltrates
C. hemorrhagic infarction
D. pleural effusion and fibrous pleuritis
E. pulmonary vasculature occluded by microthrombi
Correct Answer: A
Section: Pathology and Path physiology Hyaline membranes are usually seen microscopically in lungs showing diffuse alveolar damage. Grossly, the lungs are heavy, wet, and meaty. The clinical course is termed adult respiratory distress syndrome and is characterized by relative unresponsiveness to oxygen therapy. Eosinophilic inflammatory infiltrates (choice B), hemorrhagic infarction (choice C), pleural effusions (choice D), and vascular microthrombi (choice E) are not typically seen with diffuse alveolar damage.
Question 282:
A 45-year-old woman complains of gradually increasing fatigue. On physical examination she is noted to have obesity, hypertension, buffalo hump deformity of her back, moon facies, abdominal striae, and muscle weakness. Radiographic imaging studies identify an abnormality of her right adrenal gland which is then surgically resected. The intact specimen weighed 24 g. A hemisection of the gland is displayed in below figure. What is the most likely diagnosis?
A. adrenal cortical adenoma
B. Krukenberg tumor
C. multifocal infarction
D. neuroblastoma
E. pheochromocytoma
Correct Answer: A
Section: Pathology and Path physiology The adrenal gland shown in figure contains a cortical adenoma. Grossly, these neoplasms appear as well-demarcated, round to oval, yellowish, solitary nodules arising within the adrenal cortex. The surrounding nonneoplastic cortex is thinned and atrophic. The underlying medulla is normal. The associated clinical findings suggest Cushing syndrome due to excessive secretion of cortisol by the adenoma. Krukenberg tumor (choice B) is an enlarged ovary due to metastatic carcinoma. Adrenal infarcts (choice C) may be associated with certain bacterial infections and shock. The gland appears diffusely hemorrhagic and necrotic, without the formation of a discrete tumor nodule. Neuroblastoma (choice D) is an adrenal tumor of infancy. The typical gross appearance is a large, tan hemorrhagic mass. Hypercortisolemia is not seen. Apheochromocytoma (choice E) appears as a hemorrhagic, red- tan medullary tumor. Clinically, there may be signs of excessive norepinephrine secretion.
Question 283:
A 38-year-old woman with a history of 35 urinary tract infections over the past 2 years presents with another similar episode, including symptoms of dysuria and flank pain. Additional history includes one episode of a renal stone. Renal ultrasound is unremarkable. Urinalysis reveals pyuria, no RBCs, and no casts. Urine culture is positive for E. coli. Which of the following is the most likely underlying cause of this patient's urinary tract infections?
A. autosomal dominant polycystic kidney disease
B. focal segmental glomerulosclerosis
C. medullary sponge kidney (MSK)
D. minimal change disease
E. renal cell carcinoma
Correct Answer: C
Section: Pathology and Path physiology MSK is a relatively common disorder, appearing on approximately 1% of all intravenous pyelograms. It is a congenital, typically bilateral condition and almost all cases are sporadic. The pathological lesion consists of multiple cystic dilations of the medullary collecting ducts. Patients are generally asymptomatic until their third or fourth decade when secondary complications of urinary tract infections (UTIs), calculi, or hematuria may develop. The condition is usually benign and renal function is generally normal; in atypical cases, renal damage may result from secondary pyelonephritis or severe stone disease. Although UTIs and calculi may be complications of autosomal dominant polycystic kidney disease (choice A), this genetic condition is much more severe than MSK and chronic renal failure is the typical outcome. Patients usually present with many other common features, including hematuria, proteinuria, and hypertension; renal ultrasound is capable of detecting cystic disease in virtually all patients over the age of 30. Focal segmental glomerulosclerosis (choice B) typically presents as nephrotic syndrome or subnephrotic proteinuria, accompanied by hypertension and mild renal insufficiency in some cases. This disease may occur idiopathically or as a secondary manifestation of other conditions (e.g., HIV). There is no association with UTIs and diagnosis is made by biopsy. Minimal change disease (choice D) (also nil disease, lipoid nephrosis) is the leading cause of nephrotic syndrome in children. While adults may be affected, peak incidence of disease is 28 years. The distinguishing pathology is diffuse effacement of foot processes of glomerular visceral epithelial cells. Diagnosis is made by biopsy and electron microscopy analysis as glomeruli appear essentially normal on light microscopy, which is a disease-defining characteristic. Etiology is unknown although an immune dysfunction has been proposed. Increased incidence of disease in adults with lymphoproliferative malignancies has been reported. Disease is often limited to massive proteinuria and prognosis is excellent; response to corticosteroid therapy is dramatic. Renal cell carcinoma (also clear cell carcinoma) (choice E) is most common in older individuals (>60), and patients often present with symptoms of hematuria and flank pain; constitutional symptoms of cancer (e.g., fever, fatigue, weight loss) may also be reported. Additional findings may develop from any of a number of paraneoplastic syndromes connected with this malignancy; there is no association with recurrent UTIs however. CT scan is used for standard evaluation, although ultrasound is capable of detecting most lesions.
Question 284:
A 54-year-old construction worker collapses at his work site and is brought to the emergencyroom in a comatose state. His skin is dry and hot and his rectal temperature is 105癋. Which of the following is the most likely diagnosis?
A. heat cramps
B. heat exhaustion
C. heat stroke
D. malignant hyperthermia
E. pyrexia
Correct Answer: C
Section: Pathology and Path physiology Heat stroke is a life-threatening condition resulting from a failure of heat regulation. It is marked by high body core temperature and the failure of sweating. Heat cramps (choice A) are the result of the loss of fluid and electrolytes through sweating. Painful cramping of muscles can occur, but core temperature remains normal. Heat exhaustion (choice B) results from excessive sweating and failure to replace the lost fluid. This results in hypovolemia, venous pooling, and reduced cardiac output. The skin is wet and the temperature is usually normal. Heat exhaustion is not life threatening, and there is usually spontaneous recovery when the person is moved to a cool place. Malignant hyperthermia (choice D) is an inherited condition in which there is an increased temperature when the person is exposed to certain anesthetics. It has no relationship to environmental temperature. Pyrexia (choice E) is fever and is usually defined as a cytokine-mediated increase in body temperature as part of a response to disease. This results in the hypothalamus having a higher "set point" for the body's temperature.
Question 285:
A 47-year-old man has undergone a gradual personality change over the past 67 months with increasing moodiness and irritability During your examination you note some choreiform involuntary movements and also recognize some cognitive impairment. Afterward you talk to the man's brother who accompanied the patient to your office and he tells you that their father had similar problems for about a year prior to his death. If you could examine this patient's brain, which of the following would you expect to find?
A. areas of demyelination of the white matter
B. atrophy and loss of neurons of the caudate nucleus
C. loss of pigmented neurons of the substantia nigra
D. neurons ballooned with cytoplasmic vacuoles
E. selective atrophy of anterior frontal and temporal lobes
Correct Answer: B
Section: Pathology and Path physiology In Huntington's disease there is a symmetric atrophy of the caudate nuclei with a great reduction in the number of neurons. The putamen is also affected but usually less so. Areas of demyelination of white matter (choice A) are the classic finding in multiple sclerosis. Loss of pigmented neurons of the substantia nigra (choice C) is a consistent change seen in Parkinson's disease. Neurons ballooned with cytoplasmic vacuoles (choice D) may be seen in a number of lysosomal storage diseases of which Tay- Sachs disease is the classic example. Selective atrophy of anterior, frontal, and temporal lobes (choice E) is seen in Pick disease. There is a severe atrophy of the frontal and temporal lobes which can be sufficient to produce the "knife-edge" appearance characteristic of this disease.
Question 286:
A 31-year-old previously healthy woman develops pelvic inflammatory disease and subsequently undergoes a complete hysterectomy; her ovaries are left intact. Incidental findings in the myometrium are three discrete, sharply circumscribed masses that range from 4 to 8 cm in diameter and have a whitish, whorled cut surface. What would have been the most likely outcome over the next 5 years if these masses had not been removed?
A. complete regression
B. continued expansile growth
C. infiltration into surrounding tissues
D. metastasis via blood vessels
E. necrosis and hemorrhage
Correct Answer: B
Section: Pathology and Path physiology This description of the myometrial masses is consistent with leiomyomas, benign tumors of smooth muscle origin. Uterine leiomyomas are the most frequent tumor in women and are estimated to occur in up to 75% of women of reproductive age. As benign tumors, the expected outcome for such masses in a premenopausal woman would be continued expansile growth. Growth of leiomyomas is stimulated (but not initiated by) estrogen, therefore, regression (choice A) would be more probable in a woman of postmenopausal age or a younger woman who may have had her ovaries removed but is unlikely to be complete. Infiltration into surrounding tissues (choice C) and metastasis via blood vessels (choice D) are characteristics of malignant tumors only. While necrosis and hemorrhage (choice E) may rarely occur in benign neoplasms, they are quite characteristic of malignant neoplasms, as blood vessels are more numerous and are often poorly formed. Uterine leiomyomas and colonic adenomas are two of the exceptions to the general rule that benign neoplasms develop as single lesions.
Question 287:
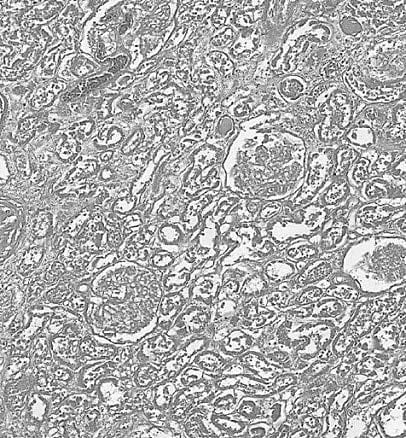
A 72-year-old woman was hospitalized after becoming acutely ill. Despite intervention, she died 9 days later. One of the findings at her autopsy is shown in below figure which is a section of her left kidney. Which of the following conditions could have led to the changes seen in this patient's kidney and was most likely the reason for her hospitalization?
A. MI
B. pyelonephritis
C. renal carcinoma
D. sepsis
E. shock
Correct Answer: A
Section: Pathology and Path physiology The photomicrograph in figure shows recognizable glomeruli and tubules but no nuclear staining, enabling one to recognize this as a renal infarct. Most renal infarcts result from thromboemboli originating in the left ventricle of a patient who has had an MI. This woman's age and her history of an acute illness leading to her death 9 days later are compatible with this sequence of events. The histology of pyelonephritis (choice B) would show viable kidney involved in an inflammatory response. Additional findings would depend upon whether it is an acute or chronic pyelonephritis. Renal carcinoma (choice C) would show viable malignant cells and not necrotic normal renal tissue. Sepsis choice D) may show indications of the infection within the renal parenchyma with an associated inflammatory response, but this is not seen in the image. Shock (choice E) is associated with acute tubular necrosis, which is a patchy necrosis affecting the proximal more than the distal tubules, but the glomeruli remain unaffected. The image shows complete necrosis of all renal elements.
Question 288:
A 27-year-old woman who recently delivered her first child develops an infiltrative mass in the anterior abdominal wall. A biopsy reveals sweeping fascicles of well-differentiated, plump monomorphic fibroblasts that infiltrate surrounding tissues. Based on this information, what is the most likely diagnosis?
A. desmoid tumor
B. fibrosarcoma
C. malignant fibrous histiocytoma
D. myositis ossificans
E. nodular fasciitis
Correct Answer: A
Section: Pathology and Path physiology Desmoid tumors are mesenchymal tumors that are locally aggressive but do not metastasize and have a benign microscopic appearance characterized by well-differentiated fibroblasts. Those tumors arising in the anterior abdominal wall are usually seen in women who are pregnant or recently postpartum. Fibrosarcomas (choice B) are rare malignant mesenchymal tumors that can metastasize and would typically be expected to have a more pleomorphic microscopic appearance (often with a "herringbone pattern") than that seen in desmoid tumors. Malignant fibrous histiocytomas (choice C) are also malignant mesenchymal tumors that would have a pleomorphic microscopic appearance. Myositis ossificans (choice D) is a non-neoplastic lesion that often forms following blunt trauma to muscle in a lower limb. The initial hematoma undergoes organization with calcification and can have a pleomorphic appearance with numerous mitoses, leading to the possibility of a misdiagnosis as a malignancy. Of special note, however, is that the bone in myositis ossificans matures from the periphery to the center, whereas the opposite pattern is seen in a malignant tumor. Nodular fasciitis (choice E) presents as a rapidly growing, potentially painful mass that may occur in association with prior trauma. Its histological appearance can be worrisome and, similar to myositis ossificans, may lead to misdiagnosis as a malignancy (sarcoma) as it is somewhat pleomorphic with immature fibroblasts and many mitoses. However, these lesions are self-limited and excision is curative.
Question 289:
A 22-year-old man recovers from a bout of hepatitis Aafter 3 weeks. One year after this infection, which of the following would a liver biopsy most likely demonstrate?
A. bridging fibrosis
B. lymphocytes spilling out of the portal tracts with piecemeal necrosis
C. lymphocytic infiltrates limited to portal triads
D. massive hepatic necrosis
E. normal histology
Correct Answer: E
Section: Pathology and Path physiology Hepatitis A does not progress to a chronic phase so one year after infection the liver histology will appear as normal. The other choices are found in active hepatitis. Bridging fibrosis (choice A) and lymphocytes spilling out of the portal tracts with piecemeal necrosis (choice B) are major features of chronic hepatitis although both can be found in severe acute hepatitis. Lymphocytic infiltrates limited to portal triads (choice C) may be seen in mild acute or chronic hepatitis. Massive hepatic necrosis (choice D) is associated with fulminant hepatitis but can also be caused by various chemical and drug toxicities.
Question 290:
Aliver biopsy of a 61-year-old man reveals the presence of clusters of cells with large, intracellular vacuoles and nuclei eccentrically displaced to the cell periphery. From which of the following conditions does this patient most likely suffer?
A. alcoholism
B. chronic liver congestion
C. hepatitis A
D. metastatic colon carcinoma E. portal vein thrombosis
Correct Answer: A
Section: Pathology and Path physiology The biopsy findings are descriptive of macrovesicular fatty change, a characteristic morphological change in the liver of patients with alcohol abuse. Morphological changes in chronic liver congestion (choice B) would demonstrate areas of centrilobular necrosis and hemorrhage, with hemosiderin-laden macrophages and varying degrees of acute inflammation. Fatty change is unusual in hepatitis A (choice C), and in most forms of hepatitis overall with the possible exception of hepatitis C, where typical morphological changes would include cellular edema, a cytoplasmic ground glass appearance, lymphocytic infiltrate, and focal or centrizonal necrosis. Histological findings for metastatic colon carcinoma (choice D) would demonstrate pleomorphic cells with hyperchromatic nuclei, and possible mitotic figures. Liver biopsy of an area with portal vein thrombosis (choice E) would reveal sinusoidal distention with areas of hemorrhage and hepatocellular atrophy.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.