Amother has brought her 3-month-old baby to the pediatrician and indicates that the infant is lethargic and has poor suckling and seems uninterested in eating. In addition, the mother notes that the baby's diapers often smell like burnt sugar. This infant likely has a defect in which of the following enzymes?
A. branched-chain alpha-keto acid dehydrogenase
B. cystathionine synthase
C. glycine cleavage complex (GCC)
D. homogentisate oxidase
E. phenylalanine hydroxylase
Correct Answer: A
Question 562:
Hemochromatosis, a disorder that is the result of excess iron accumulation, is caused by deficiencies in which of the following proteins?
A. divalent metal transporter-1 (DMT1)
B. human leukcocyte antigen (HLA) complex iron protein (HFE)
C. ferritin
D. ferroportin
E. transferrin
Correct Answer: B
Section: Biochemistry Hemochromatosis is defined as a disorder in iron metabolism that is characterized by excess iron absorption, saturation of iron-binding proteins, and deposition of hemosiderin in the tissues. The primary affected tissues are the liver, pancreas, and skin. Iron deposition in the liver leads to cirrhosis and in the pancreas causes diabetes. The excess iron deposition leads to bronze pigmentation of the organs and skin. In fact, the bronze skin pigmentation seen in hemochromatosis, coupled with the resulatant diabetes lead to the designation of this condition as bronze diabetes. The primary cause of hemochromatosis is the inheritance of an autosomal recessive allele. The locus causing hemochromatosis has been designated HFE and is a major histocompatibility complex (MHC) class-1 gene. The gene encodes an alpha-chain protein with three immunoglobulinlike domains. This alpha- chain protein associates with beta-2microglobulin. Normal HFE has been shown to form a complex with the transferrin receptor and in so doing is thought to regulate the rate of iron transfer into cells. A mutation in HFE will therefore, lead to increased iron uptake and storage. The majority of hereditary hemochromatosis patients harbor a mutation in HFE that results in the substitution of Cys 282 for a Tyr. This mutation causes loss of conformation of one of the immunoglobulin domains in HFE. Another mutation found in HFE causes a change of His68 to Asp. DMT1 (choice A) is responsible for the intestinal absorption of dietary iron and thus, a deficiency in this protein would lead toreduced total body iron, not excess. Ferritin (choice C) is the intracellular iron binding and storage protein. A deficiency in ferritinwould lead to less iron deposition, not excess. Ferroportin (choice D) is the iron transport protein that moves dietary iron from within intestinal enterocytes across the basolateral membrane to the circulation, therefore, a deficiency in this protein would have consequences similar to deficiencies in DMT1. Transferrin (choice E) is the iron transport protein of the blood that binds to the trasferrin receptor on cell surfaces, allowing cellular uptake of circulating iron. A deficiency in this protein would lead to less iron deposition not more.
Question 563:
In carrying out an assay using cultured hepatocytes, you find that addition of hemin (Fe3+ heme) does not have the expected consequence of reduced protoporphyrin IX synthesis. This result suggests that your hepatocytes harbor a mutant form of one of the heme-regulated enzymes of porphyrin biosynthesis. Which of the following represents the likely enzyme?
A. ALA dehydratase
B. ALA synthase
C. ferrochelatase
D. heme oxygenase
E. PBG deaminase
Correct Answer: B
Section: Biochemistry In the liver, hemin acts as a feedback inhibitor on ALAsynthase reducing its activity. In addition, hemin acts to repress transport of ALAsynthase into the mitochondria as well as repressing synthesis of the enzyme. Therefore, a continued synthesis of protoporphyrin IX in the presence of hemin indicates that ALA synthase is active but nonresponsive to the inhibitory action of hemin. None of the other enzymes of heme biosynthesis (choices A, CE) are inhibited by hemin.
Question 564:
A 4-year-old patient is presented in the pediatric clinic with microcytic anemia. An analysis of his blood by
nondenaturing electrophoresis reveals the following composition of hemoglobin isoforms:
HbF = 75%, HbA = 23%, HbA2 = 2%, and HbS = 0%. Using these data, is it possible to determine that the
infant is most likely homozygous for which of the following?
A. complete deletion of the alpha-globin locus
B. complete deletion of the beta-globin locus
C. mutation in the promoter of the betaglobin genes
D. nonsense mutation in the alpha-globin genes
E. nonsense mutation in the beta-globin genes
Correct Answer: C
Question 565:
Fragile X syndrome is caused by expansion of a trinucleotide repeat in the fragile X mental retardation- 1 (FMR1) gene. This disorder is characterized by which of the following symptoms?
A. accumulation of copper leading to formation of Kayser-Fleischer rings in the eyes
B. hypoketotic hypoglycemia and metabolic acidosis
C. isovaleric acidemia, severe metabolic acidosis, and neonatal fatality
D. mental retardation of severity linked to the level of trinucleotide repeat expansion
E. very long-chain fatty acid accumulation and myelin defects
Correct Answer: D
Section: Biochemistry Fragile X syndrome is the most common form of inherited mental retardation. The symptoms of this disoder are caused by a disruption in the FMR1 gene. The disruption occurs as a result of the expansion of a trinucleotide repeat sequence in the 5' untranslated region of the FMR1 gene. The severity of mental retardation in fragile X syndrome is proportional to the level of expansion of the trinucleotide repeat. Copper accumulation leading to Kayser-Fleisher rings in the eyes(choice A) is indicative of Wilson disease, which results from impaired biliary copper excretion. The symptoms of hypoketotic hypoglycemia and metabolic acidosis (choice B) are indicative of glutaric acidemia type II, which results from deficiencies in mitochondrial ubiquinone oxidoreductase. Isovaleric academia (choice C) is a severe neonatal disorder resulting from a deficiency in one of the enzymes of branched-chain amino acid metabolism, isovaleryl-CoA dehydrogenase. Accumulation of abnormally high levels of very long-chain fatty acids and defects in myelin formation (choice E) are symptoms associated with X-linked adrenoleukodystrophy (X-ALD).
Question 566:
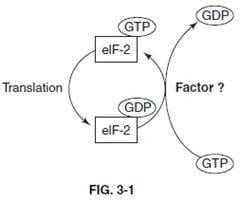
Control of the rate of translational initiation can be exerted at the level of the activity of the guanosine triphosphate (GTP)-binding and hydrolyzing initiation factor, eIF-2. The efficiency with which eIF-2 recycles between the active GTP-bound form and the inactive GDPbound form is controlled by the action of the initiation factor depicted as "Factor ?" in below figure. What is the identity of this factor?
A. eIF-1
B. eIF-2B
C. eIF-4A
D. eIF-4E
E. eIF-4G
Correct Answer: D
Section: Biochemistry The eIF-2 cycle consists of the translation initiation factors, eIF-2A and eIF-2B (also called guanine-nucleotide exchange factor, GEF). The cycle involves the binding of GTP by eIF-2A forming a complex that then interacts with the initiator methionyl-tRNA. When the initiator methionyl-tRNA is placed into the correct position of the 40S ribosomal subunit, the GTP ishydrolyzed (generating GDP and release of Pi) to provide the energy necessary to correctly position the incoming mRNA such that the initiator AUG codon and the initiator methionyltRNA anticodon are aligned. In order to regenerate an active eIF-2A for subsequent translation initiation events, the GDP must be exchanged for GTP. The exchange reaction is catalyzed by eIF-2B. The initiation factor, eIF-1 (choice A), facilitates the correct positioning of the initiator methionyltRNA and the mRNA. Initiation factor eIF-4A (choice C) binds to the mRNAand is required to "melt" any secondary structure that may exist at the 5'-end of the mRNA. Initiation factor eIF-4E (choice D) physically binds the cap structure at the 5'-end of the mRNA. Initiation factor eIF-4G (choice E) acts as a scaffold for eIF-4E facilitating cap structure binding by eIF-4E. Together, the complex composed of eIF-4A, eIF-4E, and eIF-4G is sometimes referred to as eIF-4F.
Question 567:
In Type I diabetes, the increased production of ketone bodies is primarily a result of which of the following?
A. a substantially increased rate of fatty acid oxidation by hepatocytes
B. an increase in the rate of the citric acid cycle
C. decreased cyclic adenosine monophosphate (cAMP) levels in adipocytes
D. elevated acetyl-CoA levels in skeletal muscle
E. increased gluconeogenesis
Correct Answer: A
Section: Biochemistry In fasting or diabetes, lipolysis predominates in adipocytes because of the inability of these cells to obtain glucose, which is normally used as a source of glycerol-3-phosphate. Glycerol-3-phosphate is necessary for the esterification of fatty acids into triacylglycerides. Circulating fatty acids become the predominant fuel source, and beta-oxidation in the liver becomes substantially elevated. This leads to an increased production of acetyl-CoA. Although gluconeogenesis is increased (choice E) in the liver as a result of the persistent elevation of glucagon levels, this pathway does not supply acetyl-CoA for the production of ketone bodies. The increased gluconeogenesis predisposes oxaloacetate and reduces (not increases, choice B) the flow of acetyl-CoA through the citric acid cycle. As a consequence, acetyl-CoA is diverted to the formation of ketone bodies. The persistently elevated levels of glucagon also increase the levels of cAMP in responsive tissues, such as adipocytes (choice C). This effect in adipocytes leads to persistently increased release of fatty acids to the circulation. Since skeletal muscle lacks receptors for glucagon, there is no diabetes-mediated increase in muscle metabolism and thus no elevation in acetyl-CoA levels in skeletal muscle (choice D).
Question 568:
Which of the following occurs in the lipidosis known as Tay-Sachs disease?
A. Ganglioside GM2 is not catabolized by lysosomal enzymes.
B. Phosphoglycerides accumulate in the brain.
C. Synthesis of a specific ganglioside is decreased.
D. Synthesis of a specific ganglioside is excessive.
E. Xanthomas, due to cholesterol deposition, are observed.
Correct Answer: A
Question 569:
Synthesis of glycogen is inhibited in hepatocytes in response to glucagon stimulation primarily as a result of which of the following?
A. a decrease in the level of phosphoprotein phosphatase
B. a decrease in the level of phosphorylated phosphorylase kinase
C. a decrease in the levels of phosphorylated phosphoprotein phosphatase inhibitor-1
D. an increase in the level of the dephosphorylated form of glycogen synthase
E. an increase in the level of the phosphorylated form of glycogen synthase
Correct Answer: E
Section: Biochemistry Glucagon is released from the pancreas in response to low blood glucose and stimulates hepatocytes to synthesize glucose for delivery to the blood. Therefore, it would be counterproductive for hepatocytes to divert any of the gluconeogenically derived glucose into glycogen. This is accomplished by inhibition of glycogen synthase. Glucagon exerts its effects on the liver through the glucagon receptor. When glucagon binds, the receptor activates adenylate cyclase leading to increased production of cAMP. In turn, cAMP activates cAMP-dependent protein kinase, which then phosphorylates a number of substrates. Glucagon has no effect on the level of phosphoprotein phosphatase (choice A). One of the substrates of PKA is glycogen synthase/phosphorylase kinase. Therefore, there would not be a decrease in the level of phosphorylated phosphorylase kinase (choice B). In turn, synthase/phosphorylase kinase phosphorylates glycogen phosphorylase and glycogen synthase. Therefore, there is no increase in the level of dephosphorylated glycogen synthase (choice D). Phosphorylation inhibits glycogen synthase activity and activates phosphorylase. In addition, PKA itself can phosphorylate glycogen synthase. The net effect is an increase in the rate of glucose phosphorolysis from glycogen and a reduced incorporation of glucose into glycogen. An additional PKA substrate is phosphoprotein phosphatase inhibitor-1, and therefore therewould not be a decrease in the level of the phosphorylated form of this enzyme (choice C).
Question 570:
Presentation of the platelet membrane protein complex, GPIIb-GPIIIa, which binds with von Willebrand factor, is necessary for which of the following?
A. activation of PKC leading to phosphorylation of myosin light chain and platelet morphology changes
B. cleavage and activation of high molecular weight kininogen
C. inducing platelet crosslinking
D. release of thrombin from platelet granules
E. stimulation of endothelial and smooth muscle cell interaction resulting in vasoconstriction
Correct Answer: C
Section: Biochemistry The platelet membrane glycoprotein complex, GPIIb-GPIIIa, is a receptor for fibrinogen. Presentation of GPIIb-GPIIIa on the surface of activated platelets leads to platelet crosslinking. The cross-linking occurs between activated platelets that are adhered to the endothelial cell surface via interaction of the platelet surface complex GPIa-GPIIa with exposed collagen, as well as between platelets in the local circulation. The effect is to ensure that a loose platelet plug forms rapidly at the site of vascular injury stemming the flow of blood until a fibrin clot can be formed. Activation of platelet PKC (choice A) is the consequence of thrombin binding to platelet thrombin receptors. Cleavage of high molecular weight kininogen (choice B) occurs upon the activation of factor XII. Release of thrombin from platelet alpha granules (choice D) occurs in response to platelet activation. Activation of platelets must first occur in order for GPIIb- GPIIa to be presented on the surface and, thus, this glycoprotein complex is not directly involved in platelet activation and granule release. Vasoconstriction, in concert with hemostasis (choice E), occurs primarily as a result of the action of serotonin released from alpha granules of activated platelets.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.