A family reports that their mother's mental status has been deteriorating for the past several years, during which time she has had episodes of transient weaknesses of the arms and legs. Which of the following is the most likely diagnosis?
A. Alzheimer's disease
B. Korsakoff syndrome
C. multi-infarct dementia
D. old age
E. vitamin deficiency
Correct Answer: C
Section: Behavioral Science and Biostatics Multi-infarct dementia is caused by repeated cerebrovascular ischemia, indicated in this case by periods of transient paralysis. Alzheimer's disease (choice A) is the most common primary dementia in the elderly. Old age (choice D) alone is no cause for dementia. Korsakoff syndrome (choice B), which is characterized by confabulation, is associated with alcohol withdrawal and thiamine deficiency (choice E). There is no evidence of either in this case.
Question 82:
The following are pharmacokinetic data for the drug propranolol in a 70-kg person: clearance, 50 L/h; volume of distribution, 270 L; effective plasma concentration, 20 ng/mL; oral availability (percentage), 25%. What is the oral maintenance dosing rate for propranolol in a 70-kg person?
A. 10 g/h
B. 200 g/h
C. 1 mg/h
D. 4 mg/h
E. 54 mg/h
Correct Answer: D
Section: Pharmacology The maintenance dosing rate (D/T) is calculated using the formula D/T = target ?CL/F, where D is the dose administered, T is the time interval between doses, the target is the desired steady-state plasma concentration (for which the effective plasma concentration is used), CL is the systemic clearance, and F is the fractional absorption. After multiplying the clearance (50 L/h) times the effective plasma concentration (0.02 mg/L), the resulting product of 1 mg/h must be divided by the fractional absorption of 0.25, giving a dosing rate of 4 mg/h. Note that the units for clearance and target concentration must be consistent with respect to volume. The extensive first-pass metabolism of propranolol means that to achieve the same systemic concentration, an oral dose four times larger than the IV dose must be administered.
Question 83:
At a blood alcohol level of 200 mg/dL (0.2%), which of the following correctly describes the systemic elimination process for ethanol?
A. constant clearance via liver, kidney, and lungs
B. first-order elimination via pulmonary exhalation
C. first-order elimination via renal excretion
D. second-order elimination via biliary secretion
E. zero-order elimination via hepatic metabolism
Correct Answer: E
Section: Pharmacology At a blood alcohol level of 200 mg/dL, most individuals are grossly inebriated; a level of 80100 mg/dL (0.08- 0.1%) is considered the legal threshold for intoxication in most states. Ethanol is metabolized by alcohol dehydrogenase (and to a lesser extent by the microsomal ethanol oxidizing system) to acetaldehyde, primarily in the liver. At most ethanol concentrations, the metabolizing system is saturated. As a result, zeroorder kinetics are observed. A typical adult shows a constant elimination rate manifested as a decline in blood level of 1622 mg/dL/h. As blood alcohol levels drop below about 100 mg/dL, elimination has characteristics intermediate between zero and first order. Only at concentrations below 1 mg/dL is the elimination truly first order. Constant clearance (choice A) requires first-order elimination. Pulmonary excretion (choice B) of ethanol accounts for only a minor component of elimination. Breath analyzers are used to estimate the blood alcohol level in drivers suspected of driving under the influence of alcohol. Renal excretion (choice C) also accounts for only a minor component of systemic elimination of alcohol. Because of the small size of the ethanol molecule, most of the alcohol undergoing filtration at the glomerulus is reabsorbed. Biliary secretion (choice D) is not significant in ethanol elimination. At a concentration of 200 mg/dL, blood alcohol is eliminated at zero-order kinetics via hepatic alcoholic dehydrogenase.
Question 84:
Which of the following agents is most effective as a cardiac stimulant in the treatment of severe beta-blocker overdose?
A. atrial natriuretic peptide
B. epinephrine
C. glucagon
D. human growth hormone
E. insulin
Correct Answer: C
Section: Pharmacology The cardiac manifestations of beta-blocker intoxication can be very severe, resulting in bradycardia, AV blockade, and markedly reduced force of contraction and cardiac output. Hypotension is common. However, the heart has glucagon receptors that are linked to stimulation of adenylyl cyclase independent of beta adrenoreceptors, which mediate marked increases in rate and force and substitute for the blocked beta response. (Glucagon also plays a primary role in raising blood glucose levels through activation of glycogenolysis and gluconeogenesis.) Atrial natriuretic peptide (choice A) is released from the cardiac atria and causes vasodilation through activation of membranebound guanylyl cyclase in arteriolar smooth muscle, and sodium excretion in the urine through an increase in glomerular filtration rate and consequent increase in filtration fraction. It is of no value in beta-blocker overdose. If the beta-blocker overdose is sufficient, administration of beta agonists such as epinephrine (choice B) is inadequate to overcome the blockade. Human growth hormone (choice D) is a peptide hormone produced by the anterior pituitary. It stimulates growth at open epiphyses through production of the insulin-like growth factors. It has no direct effect on cardiac function. Insulin (choice E) activates entry of glucose into most tissues and promotes glycogen and triglyceride storage. It has no direct effects on cardiac function.
Question 85:
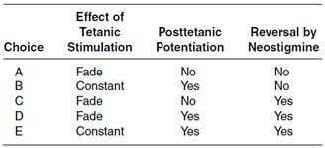
The table below provides several possible descriptions of the actions of nondepolarizing neuromuscular blockers such as tubocurarine. Which description is most accurate?
A. Option A
B. Option B
C. Option C
D. Option D
E. Option E
Correct Answer: D
Section: Pharmacology Nondepolarizing neuromuscular blockers are heavily used in anesthesia because they produce full surgical relaxation without causing significant cardiovascular depression. They act as nicotinic cholinoceptor blockers at the neuromuscular nicotinic receptor, with little or no ganglionic blockade. They have some effect on presynaptic cholinoceptors of motor nerves and it is believed that this site of action is the cause of alterations in the response of the motor nervemuscle system to rapid stimulation. A train of four stimulations, a form of titanic stimulation, is used by anesthesiologists to monitor the level of neuromuscular block in the anesthetized patient and consists of a brief period of stimulation. In the absence of drugs, as well as in the presence of a depolarizing blocker, the twitches during train of four are well maintained in strength. However, after a nondepolarizing blocker the contraction strength fades during the sequence (choices A, C, or D). In the absence of drugs, rapid tetanic stimulation results in moderate increase in contraction during the tetanus and a marked increase in strength of the muscle twitch following the end of the train due, at least in part, to a buildup of calcium in the motor nerve terminal. This posttetanic potentiation is enhanced by nondepolarizing blockers (choices B, D, or E). Finally, nondepolarizing blockade results from competitive blockade of cholinoceptors, so increasing the amount of acetylcholine in the synapse by means of a drug like neostigmine can reverse the blockade (choices C, D, or E). Thus, only choice D meets all three requirements.
Question 86:
Which of the following is the best treatment for uncomplicated primary syphilis?
A. ciprofloxacin
B. clarithromycin
C. doxycycline
D. gentamycin
E. penicillin G
Correct Answer: E
Section: Pharmacology Penicillin is still the treatment of choice for treponemal infections due to continuing sensitivity in most areas and low toxicity. The other drugs listed (choices AD) offer no advantages and greater risk of lack of responsiveness and greater toxicity.
Question 87:
Which of the following associates the correct mechanism of action with a drug used in Type II (noninsulindependent) diabetes?
A. acarbose--reduction of insulin resistance
B. glipizide--inhibition of intestinal alphaglucosidase
C. metformin--inhibition of ATP-sensitive potassium channels
D. repaglinide--modulation of pancreatic insulin release
E. rosiglitazone--reduction in circulating glucagon levels
Correct Answer: D
Section: Pharmacology Pancreatic beta cells are electrically polarized. Depolarization causes entry of calcium and activation of insulin exocytosis. In hypoglycemia, the negative resting potential is maintained by the activity of an ATP-sensitive hyperpolarizing potassium channel and insulin secretion is inhibited. When extracellular glucose levels are high, glucose enters the beta cells via the GLUT2 transporter and is metabolized to yield ATP. The increased ATP levels cause closure of the potassium channel, allowing the cell to depolarize and secrete insulin. Modulation of insulin release (choice D) is the mechanism of action of the meglitinides such as repaglinide. Although the details are not fully understood, these drugs share one binding site with sulfonylureas and have a second, independent binding site. Acarbose (choice A) is an inhibitor of intestinal alpha-glucosidase and thus reduces absorption of glucose. Sulfonylureas such as glipizide (choice B) bind to a cell-surface protein to cause inhibition of the hyperpolarizing potassium channel, thereby allowing the beta cell to depolarize and secrete insulin. Metformin (choice C) and other biguanides are poorly understood, but do not inhibit the potassium channel that is the target of sulfonylureas. Rosiglitazone (choice E) and pioglitazone do not act by reduction of circulating glucagon; this is one proposed mechanism for the biguanides. These thiazolidinediones or "glitazones" appear to act by a peripheral mechanism that reduces insulin resistance, probably mediated by the peroxisome proliferator-activated receptor-gamma (PPAR-gamma) nuclear receptor.
Question 88:
The mechanism of anesthetic action for lidocaine involves which of the following?
A. blockade of axonal voltage-dependent calcium channels
B. blockade of axonal voltage-dependent sodium channels
C. hyperpolarization of axons via enhanced chloride influx
D. hyperpolarization of axons via enhanced potassium efflux
E. inhibition of nerve terminal pain receptors
Correct Answer: B
Section: Pharmacology Local anesthetic agents such as lidocaine inhibit nerve conduction through state- and use-dependent blockade of voltage-dependent fast sodium channels. As a result, the threshold of excitability of the nerve is increased, and the ability of the nerve to propagate an action potential is decreased. Ultimately, transmission of sensory stimuli to the CNS is suppressed, and motor function involving small fibers in the vicinity of the injection is also lost. Inhibition of nerve conduction via blockade of calcium channels (choice A) is not a mechanism for local anesthetic agents. Hyperpolarization of neurons via enhanced chloride influx (choice C) is not a mechanism for local anesthetic agents, but is the mechanism for inhibition of repetitive neuronal firing by the benzodiazepines, barbiturates, and other GABA-mimetic and -enhancing agents that act on the GABAA receptor-chloride channel of neurons. Enhanced potassium efflux (choice D) does not occur with local anesthetics. Inhibition of pain receptors (choice E) is not a mechanism for currently available analgesic agents, although antagonists at the neurokinin receptors involved in nociception (pain perception) are an area of intense research.
Question 89:
Which of the following is the current drug of choice for treatment of roundworm (Ascaris) infections?
A. diethylcarbamazine
B. ivermectin
C. mebendazole
D. niclosamide
E. praziquantel
Correct Answer: C
Section: Pharmacology Mebendazole is a broad-spectrum antihelmintic that is effective against a variety of nematodes including ascarids, hookworm (Necator, Ancylostoma), whipworm (Trichuris), threadworm (Strongyloides), and pinworm (Enterobius). Adverse effects are rare. Diethylcarbamazine (choice A) was developed as a treatment for filariasis. Because of adverse effects that include nausea, vomiting, headache, leukocytosis, and proteinuria, it has been largely supplanted by other antifilarial agents, except in the case of Loa loa, where it remains the drug of choice. Ivermectin (choice B) is used to treat Onchocerca volvulus, the agent responsible for river blindness in west and central Africa. Niclosamide (choice D) and praziquantel (choice E) are agents with primary efficacy against flukes and tapeworms. In the case of Fasciola hepatica (sheep liver fluke), however, bithionol or triclabendazole (a veterinary drug) are drugs of choice; in cysticercosis, albendazole is the drug of choice.
Question 90:
Calcium disodium edetate is most effective as an antidote for poisoning with which of the following?
A. arsenic
B. atropine
C. iron
D. lead
E. mercury
Correct Answer: D
Section: Pharmacology Chronic lead poisoning results in multiple toxicities including headache, hypertension, infertility, anemia, and renal insufficiency. Mental and growth retardation occur in children. Acute lead intoxication usually presents as encephalopathy or severe abdominal colic, sometimes masquerading as pancreatitis. When blood lead levels exceed 50 mcg/dL, chelation treatment is indicated. The calcium ion in calcium disodium edetate (EDTA) is readily displaced by lead, forming a lead chelate that is excreted in the urine. Arsenic poisoning (choice A) is treated with chelation therapy using dimercaprol, succimer, or penicillamine. Atropine (choice B) is a lipophilic muscarinic receptor antagonist that blocks parasympathetic function and at toxic levels produces hallucinations and psychosis. Treatment of atropine intoxication consists of symptomatic management or administration of the lipid-soluble nticholinesterase physostigmine. Toxicity from iron (choice C) may arise from ingestion of iron supplements (as with children swallowing adult preparations) or hemolytic diseases such as thalassemia. Treatment consists of the use of the iron-chelating agents deferoxamine or deferasirox. EDTA does not chelate mercury (choice E). Inorganic mercury poisoning is treated by using chelation therapy with dimercaprol, succimer, or penicillamine. Organic mercury poisoning is more difficult to treat because of the lipophilic nature of organomercury compounds.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-1 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.