Which of the following is a degenerative disease of the central nervous system (CNS) caused by infectious proteins called prions?
A. Creutzfeldt-Jakob disease (CJD)
B. Alzheimer's disease
C. Parkinson's disease
D. Cushing disease
E. Guillain-Barr?syndrome
Correct Answer: A
CJD is caused by an infectious protein called a prion. Patients typically are between 50 and 75 years of age and present with dementia and clonus. The disease is progressive and death occurs generally within a year of symptom onset. CJD is found throughout the world, and no consistent etiologic agent has been identified.
Question 62:
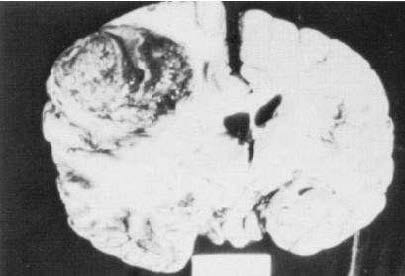
A 57-year-old man complains of worsening headache, nausea, and vomiting for 2 months. On examination, he is lethargic, confused, and has right-sided weakness. While waiting for a computed tomography (CT) scan, he develops status epilepticus, suffers cardiorespiratory arrest, and dies. His brain at autopsy is shown in the figure below. Which of the following is the most likely diagnosis?
A. glioma
B. meningioma
C. craniopharyngioma
D. pituitary adenoma
E. acoustic neuroma
Correct Answer: A
The autopsy specimen illustrated in Figure contains a large, multicolored, irregular tumor invading the left hemisphere. There is hemorrhage, necrosis, and surrounding edema. The clinical and pathologic findings are most compatible with a diagnosis of malignant glioma (astrocytoma). Glioma is a highly malignant tumor of astrocytic cells and is the most common primary brain tumor. It infiltrates widely, often involving multiple lobes, as well as the opposite hemisphere via the corpus callosum. Prognosis is poor, with an average survival time of 6 months after diagnosis. Meningiomas are benign primary brain tumors that are usually slow growing and occur outside of the hemispheres, where they are well encapsulated and compressed but do not invade brain tissue. Craniopharyngiomas arise from remnants of Rathke's pouch (the craniopharyngeal anlage). They are usually benign, well encapsulated, and found in or near the sella turcica. Acoustic neuromas arise from the root of the eighth cranial nerve in the cerebellopontine angle. Like meningiomas, they are encapsulated and compressed rather than invade brain substance
Question 63:
A dentist asks you to evaluate a 42-year-old woman before tooth extraction. In patients who are not intravenous (IV) drug users and who do not have prosthetic valves, which of the following organisms is the most common cause of bacterial endocarditis?
A. Enterococcus
B. Streptococcus
C. gram-negative bacilli
D. Candida
E. Pseudomonas
Correct Answer: B
Guidelines for antibiotic prophylaxis of infective endocarditis (IE) underwent a major revision in 2007. Prophylaxis is now only recommended for those patients at highest risk of IE including patients with a prosthetic valve, history of IE, cardiac transplant patients that develop valvulopathy, cyanotic congenital heart disease that remains unrepaired, cyanotic congenital heart disease that has been repaired with a prosthesis during the first 6 months after the procedure or if a defect remains at the site of the prosthesis after 6 months. Congestive heart failure, an S4 gallop, and diabetes do not increase risk. Recommended antibiotic coverage for high-risk patients before dental procedures is amoxicillin 2 g PO 1 hour before the procedures. Penicillin-allergic patients can receive clarithromycin, cephalexin, cefadroxil, or clindamycin as prophylaxis. Streptococci and S. aureus are responsible for the majority of community- acquired native valve endocarditis cases.
In IV drug abusers, S. aureus is responsible for more than 50% of cases, and Candida and Pseudomonas for about 6% each. Patients with prior endocarditis are at high risk. Bacterial endocarditis carries a mortality rate of about 25%, and prevention is of paramount importance. In S. aureus endocarditis in injection drug users, mortality is only 1015%. As many as 40% of cases occur without underlying heart disease. VSD, patent ductus arteriosus, and tetralogy of Fallot are most commonly associated; whereas, ASD is rarely a predisposing factor.
Question 64:
A 47-year-old man with diabetes and hypertension travels with his family to Mexico. The next morning after eating out at a local restaurant and despite drinking bottled water, he develops severe crampy abdominal pain and watery, frequent diarrhea. Which of the following is the best approach for his care?
A. ciprofloxacin . 3 days
B. penicillin . 5 days
C. tetracycline . 3 days
D. observation of symptoms
E. metronidazole . 10 days
Correct Answer: A
Ciprofloxacin is the drug of choice in a dose of 500 mg bid for 13 days because most cases of travelers' diarrhea are from E. coli. This patient's symptoms are moderate to severe and warrant antibiotic treatment which will decrease the frequency of bowel movements and duration of illness. Erythromycin and tetracycline are effective for Vibrio which is an uncommon cause of travelers' diarrhea. Metronidazole is used for Clostridium difficile enteritis.
Question 65:
A 50-year-old woman with a history of essential hypertension presents to the emergency department with sudden onset of a severe headache, nausea and vomiting, and photophobia. On examination, her BP is 160/100 mmHg. She is mildly confused and has nuchal rigidity, without focal neurologic signs. Once the diagnosis has been confirmed, which of the following is the next most important step in patient management?
A. admission to the ICU, close monitoring, and aggressive treatment of hypertension
B. urgent surgical intervention with aneurysm clipping
C. admission to the ICU, close monitoring, and IV antibiotics
D. serial lumbar punctures to drain cerebrospinal fluid (CSF)
E. anticoagulation and antiplatelet therapy
Correct Answer: B
Ruptured cerebral aneurysms often occur in the setting of hypertension. The severe headache, nausea and vomiting, photophobia, and nuchal rigidity are the result of meningeal irritation from subarachnoid blood. Subarachnoid hemorrhage is visualized on CT scan, with definitive diagnosis of the aneurysm and its location by cerebral angiography. Early surgical clipping is the current neurosurgical approach because of the significant risk of rebleeding in the first 24 hours after initial presentation. Hydrocephalus may occur as a late complication of subarachnoid hemorrhage and require serial lumbar puncture to drain CSF and control ICP. A hemorrhagic stroke can occur in association with malignant hypertension and may have concurrent subarachnoid hemorrhage. Focal neurologic signs are usually present. Meningitis will produce similar signs of meningeal irritation, but usually with other systemic signs of infection and a clinical prodromesuggesting an infectious etiology. Lumbar puncture is diagnostic, and if a bacterial source is suspected, systemic antibiotics are initiated pending culture of CSF. Ischemic cerebrovascular accidents and transient ischemic attacks are not associated with subarachnoid hemorrhage and, hence, do not present with signs of meningeal irritation. Focal neurologic signs are usually present. Evaluation of a possible cause includes Doppler examination of the carotid arteries. Management includes anticoagulation and antiplatelet therapy. EEG measures brain electrical activity and is indicated in the diagnostic evaluation of seizures.
Question 66:
A 50-year-old woman with a history of essential hypertension presents to the emergency department with
sudden onset of a severe headache, nausea and vomiting, and photophobia. On examination, her BP is
160/100 mmHg. She is mildly confused and has nuchal rigidity, without focal neurologic signs.
Which of the following is the most likely diagnosis?
A. meningitis
B. ruptured cerebral aneurysm
C. hemorrhagic stroke
D. ischemic cerebrovascular accident
E. transient ischemic attack
Correct Answer: B
Ruptured cerebral aneurysms often occur in the setting of hypertension. The severe headache, nausea and vomiting, photophobia, and nuchal rigidity are the result of meningeal irritation from subarachnoid blood. Subarachnoid hemorrhage is visualized on CT scan, with definitive diagnosis of the aneurysm and its location by cerebral angiography. Early surgical clipping is the current neurosurgical approach because of the significant risk of rebleeding in the first 24 hours after initial presentation. Hydrocephalus may occur as a late complication of subarachnoid hemorrhage and require serial lumbar puncture to drain CSF and control ICP. A hemorrhagic stroke can occur in association with malignant hypertension and may have concurrent subarachnoid hemorrhage. Focal neurologic signs are usually present. Meningitis will produce similar signs of meningeal irritation, but usually with other systemic signs of infection and a clinical prodromesuggesting an infectious etiology. Lumbar puncture is diagnostic, and if a bacterial source is suspected, systemic antibiotics are initiated pending culture of CSF. Ischemic cerebrovascular accidents and transient ischemic attacks are not associated with subarachnoid hemorrhage and, hence, do not present with signs of meningeal irritation. Focal neurologic signs are usually present. Evaluation of a possible cause includes Doppler examination of the carotid arteries. Management includes anticoagulation and antiplatelet therapy. EEG measures brain electrical activity and is indicated in the diagnostic evaluation of seizures.
Question 67:
A40-year-old alcoholic is brought to the emergency epartment with frostbite to both lower extremities. His core body temperature is 36°C. hich of the followin g is the most appropriate initial treatment for the patient's thermal injury?
A. sympathectomy without any delay
B. debridement of devitalized tissues
C. slow rewarming at room temperature
D. slow rewarming with dry heat
E. rapid rewarming in warm water
Correct Answer: E
Frostbite is produced by formation of ice crystals in the tissue, with cessation of tissue perfusion. Appropriate initial treatment is rapid rewarming in warm water, to minimize further tissue damage. Dry heat can cause further tissue damage. With reperfusion, there is continuedprogression of tissue injury because of progressive microcirculatory thrombosis. Therefore, nonviable tissue should be allowed to demarcate over several weeks, with delayed debridement. A sympathectomy is not indicated acutely, because the vasculature in frozen tissue is already maximally dilated.
Question 68:
A 19-year-old previously healthy man is an unbelted driver of a motor vehicle involved in a front-end collision. On arrival in the emergency department, the patient is noted to have stridor, with marked respiratory distress, and an oxygen saturation of 88% despite 100% oxygen by mask. He has obvious extensive facial injuries, a flail chest, and poor chest expansion. Bag-mask-valve ventilation is ineffective. Which of the following is the most appropriate next step in management?
A. orotracheal intubation
B. nasotracheal intubation
C. cricothyroidotomy
D. tracheostomy
E. placement of bilateral chest tubes
Correct Answer: C
This patient has an obstructed airway from maxillofacial trauma. The patient is stridorous, hypoxic, and cannot be ventilated with bag andf mask. Immediate cricothyroidotomy is lifesaving. In the presence of severe facial trauma, orotracheal intubation is likely to be difficult because of distortion of landmarks and excessive oropharyngeal secretions. Nasotracheal intubation is contraindicated in this setting. A definitive tracheostomy is more time consuming than a cricothyroidotomy and requires specific surgical expertise. Stabilization of the airway is the first resuscitation priority, before placement of chest tubes to relieve potential pneumothoraces.
Question 69:
A 70-year-old man is admitted to the ICU after repair of an abdominal aortic aneurysm. He has a prior history of hypertension and mild congestive heart failure, which were adequately controlled with digoxin and diuretics. To facilitate perioperative management, a Swan-Ganz (multilumen pulmonary artery) catheter was inserted in the operating room. During the first few hours postoperatively, the patient is noted to have a blood pressure of 140/70 mmHg, heart rate of 110/min, flat neck veins, a pulmonary arterial wedge pressure of 9 mmHg, and poor urine output. Several hours after this intervention, the patient is reassessed. The blood pressure is 150/85 mmHg, heart rate is 90/min, neck veins are distended, and the pulmonary arterial wedge pressure is 17 mmHg. Urine output is still low in volume. At this point, management should be which of the following?
A. IV furosemide
B. a bolus of IV crystalloid
C. a dopamine infusion
D. a nitroprusside infusion
E. IV digoxin administration
Correct Answer: D
In the initial postoperative period, the patient has a low pulmonary artery wedge pressure and poor urine output. Renal perfusion is compromised by hypovolemia, with subsequent inadequate preload and decreased cardiac output. The appropriate therapeutic intervention at this time is further IV fluid resuscitation. Diuretics are contraindicated in the patient with hypovolemia and are unlikely to improve urine output in the face of inadequate renal perfusion. A dopamine infusion or digoxin may improve cardiac contractility but will not result in improvement in cardiac output unless there is adequate preload. In a hypovolemic patient, nitroprusside will result in a significant drop in blood pressure. After receiving a fluid bolus, the patient develops distended neck veins and an elevated pulmonary wedge pressure, indicating biventricular dysfunction with increased left ventricular end-diastolic pressure, and increased left ventricular endsystolic volume. Cardiac output is low, and urine output has not improved. In a patient with a history of hypertension, this clinical picture is often caused by increased afterload. Afterload reduction can be obtained with a nitroprusside infusion.
Question 70:
A 70-year-old man is admitted to the ICU after repair of an abdominal aortic aneurysm. He has a prior history of hypertension and mild congestive heart failure, which were adequately controlled with digoxin and diuretics. To facilitate perioperative management, a Swan-Ganz (multilumen pulmonary artery) catheter was inserted in the operating room. During the first few hours postoperatively, the patient is noted to have a blood pressure of 140/70 mmHg, heart rate of 110/min, flat neck veins, a pulmonary arterial wedge pressure of 9 mmHg, and poor urine output. Which of the following is the most appropriate next step in management of this patient?
A. IV furosemide
B. a bolus of IV crystalloid
C. a dopamine infusion
D. a nitroprusside infusion
E. IV digoxin administration
Correct Answer: B
In the initial postoperative period, the patient has a low pulmonary artery wedge pressure and poor urine output. Renal perfusion is compromised by hypovolemia, with subsequent inadequate preload and decreased cardiac output. The appropriate therapeutic intervention at this time is further IV fluid resuscitation. Diuretics are contraindicated in the patient with hypovolemia and are unlikely to improve urine output in the face of inadequate renal perfusion. A dopamine infusion or digoxin may improve cardiac contractility but will not result in improvement in cardiac output unless there is adequate preload. In a hypovolemic patient, nitroprusside will result in a significant drop in blood pressure. After receiving a fluid bolus, the patient develops distended neck veins and an elevated pulmonary wedge pressure, indicating biventricular dysfunction with increased left ventricular end-diastolic pressure, and increased left ventricular endsystolic volume. Cardiac output is low, and urine output has not improved. In a patient with a history of hypertension, this clinical picture is often caused by increased afterload. Afterload reduction can be obtained with a nitroprusside infusion.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.