A64-year-old man with hypertension presents for routine follow-up of his blood pressure. His home blood pressure log reveals readings in the 150/70 range. His home monitor had previously been verified by clinic BP readings. He denies any complaints. His current medications include HCTZ 25 mg daily, metoprolol 100 mg twice daily, enalapril 20 mg twice daily, and amlodipine 10 mg daily. He states he is adherent to his medication, drug, and exercise regimen as you recommended. At this time, how would you advise the patient?
A. You need to take another blood pressure medication.
B. I need to order some tests to look for secondary causes of high blood pressure.
C. In spite of your efforts, you need to exercise more and lose more weight.
D. Your blood pressure is acceptable where it is. Continue your current regimen.
E. I need to refer you to a cardiologist.
Correct Answer: B Section: (none)
Explanation:
Resistant hypertension is defined as blood pressure not at goal despite adequate doses of a three-drug regimen including a diuretic. One of the first considerations is medication compliance and white coat hypertension. White coat hypertension can be assessed by the use of ambulatory blood pressure monitoring. A patient's home monitor should be assessed for accuracy against the office monitor. The patient's technique should also be verified. One should also assess for other agents that may lead to resistant hypertension despite pharmacologic therapy (e.g., tobacco use, NSAIDs, steroids, recreational drugs, oral decongestants, herbal medications). If the above are ruled out, one should initiate a workup to assess for a secondary cause for the hypertension, which may include chronic kidney disease, coarctation of the aorta, Cushing syndrome, steroid treatment, drug-induced hypertension, pheochromocytoma, primary aldosteronism, renovascular hypertension, sleep apnea, and thyroid/ parathyroid disease.
Question 682:
A24-year-old female presents to your office for excision of a nevus. After obtaining consent and prepping the site, you anesthetize the area with 1% lidocaine. However, as you start the procedure, you note that the patient is not sufficiently anesthetized. Your partner suggests the use of lidocaine with epinephrine. The addition of epinephrine with local anesthetics is useful because of which of the following properties?
A. It prolongs and increases the depth of local anesthesia.
B. It neutralizes the irritant action of the local anesthetic agent.
C. It increases the rate of systemic absorption and therefore hastens the onset of action of the anesthetic agent.
D. It increases the pH of the anesthetic so that less anesthetic is required to produce nerve block.
E. It blocks neurotransmitter release (thus decreasing pain perception) via stimulation of presynaptic alpha-adrenergic receptors.
Correct Answer: A Section: (none)
Explanation:
The duration of action of a local anesthetic is proportional to its contact time with the nerves. Therefore, if the drug can be localized at the nerve, the period of analgesia should be prolonged. Using a vasoconstrictor such as epinephrine decreases the systemic absorption of the local anesthetic. Once the absorption is decreased, the anesthetic remains longer at the desired site and is systemically absorbed at a slower rate, which allows destruction by enzymes and less systemic toxicity.
Question 683:
A 43-year-old patient presents with his fourth episode of culture-proven shingles in a T7 distribution. What is the most likely associated underlying condition?
A. leukemia
B. lymphoma
C. acquired immunodeficiency syndrome (AIDS)
D. chro
Correct Answer: C Section: (none)
Explanation:
The incidence and severity of shingles is increased in most immunosuppressed patients. This population includes patients with lymphoma, leukemia, or HIV; patients who have received bone marrow transplantation; and patients on chronic immunosuppressive therapy. However, HIV patients are notable for their tendency to suffer multiple recurrences of shingles.
Question 684:
A20-year-old male has had a recent wide local excision of a 1.5 mm melanoma from the right ankle. There is no evidence of metastatic disease. The most important prognostic factor for this patient is which of the following?
Which of the following is true regarding melanoma?
A. Chest radiographs are not recommended as a part of a patient's follow-up surveillance.
B. Timely treatment of metastatic melanoma has been shown to have an effect on mean survival.
C. Elevated serum LDH suggests metastatic melanoma.
D. Patients without clinical lymphadenopathy are not at risk for metastatic involvement.
E. High mitotic rate and a lower Clark level are poor prognostic signs.
Correct Answer: C Section: (none)
Explanation:
In patients who have melanoma that is confined to the skin (i.e., no evidence of metastatic disease), the most important prognostic factor is the Breslow histologic depth of the tumor. The age of the patient and location of the tumor also play a role in prognosis, but to a lesser degree. The forearm and leg tend to have a better prognosis; scalp, hands, feet, and mucous membranes have a worse prognosis. Older persons tend to have poorer prognoses, as well. Standard treatment for melanoma involves surgical excision. Sentinel lymph node biopsy should also be performed in any patient who has a melanoma that is at least 1 mm thick. This aids in determining whether melanoma cells have metastasized to the local lymph node basin. If the sentinel lymph node biopsy is negative for melanoma cells, no further lymph node studies are necessary. However, a positive biopsy warrants complete lymph node dissection. In addition to this situation, complete lymph node dissection is indicated in the setting of clinical lymphadenopathy regardless of evident distant metastasis. High dose interferon alpha-2 therapy is aviable option for use as adjuvant therapy in patients at high risk for disease recurrence, having been shown to prolong periods of remission and possibly improve mortality. Single-agent chemotherapy is generally used in patients with stage IV melanoma and is considered more for palliative purposes.
Question 685:
A20-year-old male has had a recent wide local excision of a 1.5 mm melanoma from the right ankle. There is no evidence of metastatic disease. The most important prognostic factor for this patient is which of the following? One year after his initial diagnosis and treatment, the patient develops a palpable right inguinal lymph node. Inguinal lymph node dissection reveals one node positive for metastatic melanoma; the remaining nodes are negative. Acomplete restaging workup shows no evidence of any additional metastatic disease. What is the correct stage for this patient?
A. stage I
B. stage IIa
C. stage IIb
D. stage III
E. stage IV
Correct Answer: D Section: (none)
Explanation:
In patients who have melanoma that is confined to the skin (i.e., no evidence of metastatic disease), the most important prognostic factor is the Breslow histologic depth of the tumor. The age of the patient and location of the tumor also play a role in prognosis, but to a lesser degree. The forearm and leg tend to have a better prognosis; scalp, hands, feet, and mucous membranes have a worse prognosis. Older persons tend to have poorer prognoses, as well. Standard treatment for melanoma involves surgical excision. Sentinel lymph node biopsy should also be performed in any patient who has a melanoma that is at least 1 mm thick. This aids in determining whether melanoma cells have metastasized to the local lymph node basin. If the sentinel lymph node biopsy is negative for melanoma cells, no further lymph node studies are necessary. However, a positive biopsy warrants complete lymph node dissection. In addition to this situation, complete lymph node dissection is indicated in the setting of clinical lymphadenopathy regardless of evident distant metastasis. High dose interferon alpha-2 therapy is aviable option for use as adjuvant therapy in patients at high risk for disease recurrence, having been shown to prolong periods of remission and possibly improve mortality. Single-agent chemotherapy is generally used in patients with stage IV melanoma and is considered more for palliative purposes.
Question 686:
A20-year-old male has had a recent wide local excision of a 1.5 mm melanoma from the right ankle. There is no evidence of metastatic disease. The most important prognostic factor for this patient is which of the following? Which of the following interventions is most appropriate in addition to wide local excision of the patient's melanoma?
A. sentinel lymph node biopsy
B. no further intervention is warranted
C. adjuvant therapy with interferon alpha-2 for 1 year
D. single-agent chemotherapy
E. complete lymph node dissection
Correct Answer: A Section: (none)
Explanation:
In patients who have melanoma that is confined to the skin (i.e., no evidence of metastatic disease), the most important prognostic factor is the Breslow histologic depth of the tumor. The age of the patient and location of the tumor also play a role in prognosis, but to a lesser degree. The forearm and leg tend to have a better prognosis; scalp, hands, feet, and mucous membranes have a worse prognosis. Older persons tend to have poorer prognoses, as well. Standard treatment for melanoma involves surgical excision. Sentinel lymph node biopsy should also be performed in any patient who has a melanoma that is at least 1 mm thick. This aids in determining whether melanoma cells have metastasized to the local lymph node basin. If the sentinel lymph node biopsy is negative for melanoma cells, no further lymph node studies are necessary. However, a positive biopsy warrants complete lymph node dissection. In addition to this situation, complete lymph node dissection is indicated in the setting of clinical lymphadenopathy regardless of evident distant metastasis. High dose interferon alpha-2 therapy is aviable option for use as adjuvant therapy in patients at high risk for disease recurrence, having been shown to prolong periods of remission and possibly improve mortality. Single-agent chemotherapy is generally used in patients with stage IV melanoma and is considered more for palliative purposes.
Question 687:
A20-year-old male has had a recent wide local excision of a 1.5 mm melanoma from the right ankle. There is no evidence of metastatic disease. The most important prognostic factor for this patient is which of the following?
A. the Breslow depth of the tumor
B. the Clark level of the tumor
C. the location of the tumor
D. the age of the patient
E. the number of prior severe blistering sunburns
Correct Answer: A Section: (none)
Explanation:
In patients who have melanoma that is confined to the skin (i.e., no evidence of metastatic disease), the most important prognostic factor is the Breslow histologic depth of the tumor. The age of the patient and location of the tumor also play a role in prognosis, but to a lesser degree. The forearm and leg tend to have a better prognosis; scalp, hands, feet, and mucous membranes have a worse prognosis. Older persons tend to have poorer prognoses, as well. Standard treatment for melanoma involves surgical excision. Sentinel lymph node biopsy should also be performed in any patient who has a melanoma that is at least 1 mm thick. This aids in determining whether melanoma cells have metastasized to the local lymph node basin. If the sentinel lymph node biopsy is negative for melanoma cells, no further lymph node studies are necessary. However, a positive biopsy warrants complete lymph node dissection. In addition to this situation, complete lymph node dissection is indicated in the setting of clinical lymphadenopathy regardless of evident distant metastasis. High dose interferon alpha-2 therapy is aviable option for use as adjuvant therapy in patients at high risk for disease recurrence, having been shown to prolong periods of remission and possibly improve mortality. Single-agent chemotherapy is generally used in patients with stage IV melanoma and is considered more for palliative purposes.
Question 688:
A 45-year-old male has received intravenous contrast dye prior to CT scan of the abdomen. Twenty minutes later the patient reports severe pruritus. He denies respiratory distress, syncope, or palpitations. His blood pressure is 98/54, pulse is 90, and respiratory rate is 22. On physical examination, he has widespread urticaria. His lungs are clear to auscultation. The next appropriate step would be which of the following This intervention works well in cases such as this due to activity directed toward which of these receptors?
A. dopaminergic receptors
B. muscarinic receptors
C. nicotinic receptors
D. adrenergic receptors
E. N-methyl D-aspartate (NMDA) receptors
Correct Answer: D Section: (none)
Explanation:
Anaphylaxis is an acute multisystem allergic reaction to a particular antigen in a sensitized patient. The reaction may be mild or severe. Clinical manifestations may include urticaria and angioedema; laryngeal edema with dyspnea; bronchospasm; tachycardia and hypotension; and vomiting and diarrhea. The correct initial step in the treatment of mild anaphylaxis is the administration of 0.30.5 mL of 1:1000 epinephrine subcutaneously. (Kaspar et al., 2005, pp. 19491950) Epinephrine is the drug of choice for treating severe anaphylactic shock because it is active at both alpha-and beta-adrenergic receptors. The alphaadrenergic effects constrict the smaller arterioles and precapillary sphincters, thereby markedly reducing cutaneous blood flow. Veins and large arteries also respond to epinephrine. The beta-adrenergic effects of epinephrine cause relaxation of the bronchial smooth muscle and induce a powerful bronchodilation, which is most evident when the bronchial muscle is contracted, as in anaphylactic shock
Question 689:
A 45-year-old male has received intravenous contrast dye prior to CT scan of the abdomen. Twenty minutes later the patient reports severe pruritus. He denies respiratory distress, syncope, or palpitations. His blood pressure is 98/54, pulse is 90, and respiratory rate is 22. On physical examination, he has widespread urticaria. His lungs are clear to auscultation. The next appropriate step would be which of the following?
A. administration of 0.5 mL of 1:1000 epinephrine subcutaneously
B. administration of 0.5 mL of 1:100,000 epinephrine subcutaneously
C. administration of 25 mg of diphenhydramine subcutaneously
D. administration of intravenous glucocorticoids
E. careful observation but no medications
Correct Answer: A Section: (none)
Explanation:
Anaphylaxis is an acute multisystem allergic reaction to a particular antigen in a sensitized patient. The reaction may be mild or severe. Clinical manifestations may include urticaria and angioedema; laryngeal edema with dyspnea; bronchospasm; tachycardia and hypotension; and vomiting and diarrhea. The correct initial step in the treatment of mild anaphylaxis is the administration of 0.30.5 mL of 1:1000 epinephrine subcutaneously. (Kaspar et al., 2005, pp. 19491950) Epinephrine is the drug of choice for treating severe anaphylactic shock because it is active at both alpha-and beta-adrenergic receptors. The alphaadrenergic effects constrict the smaller arterioles and precapillary sphincters, thereby markedly reducing cutaneous blood flow. Veins and large arteries also respond to epinephrine. The beta-adrenergic effects of epinephrine cause relaxation of the bronchial smooth muscle and induce a powerful bronchodilation, which is most evident when the bronchial muscle is contracted, as in anaphylactic shock
Question 690:
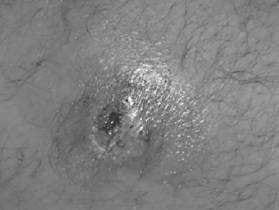
A23-year-old presents with the history of a suspected spider bite to the left groin. On questioning, no one saw a spider. The patient has been healthy except occasional boils under his arms and in the groin. The patient is afebrile. No family members are sick.
The patient is sent home and a day later develops chills, fever, and the lesion is spreading. Appropriate treatment would include which of the following?
A. hospital admission, blood cultures, and vancomycin
B. systemic corticosteroids
C. surgical excision of any necrotic tissue
D. observation and monitoring at home with oral clindamycin
E. hospital admission, blood cultures, and ceftriaxone
Correct Answer: A Section: (none)
Explanation: Above shows a pustule or furuncle with a necrotic center. With the patient having a history of boils under his arms and groin, a S. aureus infection should be suspected. Communityacquired methicillin-resistant S. aureus (MRSA) infection has been described to present as an appearance similar to a spider bite. Brown recluse spider bites have necrotic centers, but do not usually form pustules. TMP-SMZ is the best oral agent available for MRSA. Benadryl and topical steroids would not be indicated. Surgical debridement is not indicated. If there is a large pustule, incision and drainage of the wound may be useful. Alternatively, a needle aspirant of drainage could be sent for culture. Patients should be instructed not to press on these lesions to express puss. This causes bacterimia and can later lead to serious systemic infections due to S. aureus. If a patient with S. aureus infection becomes febrile, he should be admitted to the hospital for systemic antibiotics. Blood cultures should be taken. S. aureus easily forms abscesses in the skin and in other tissues. Blood-borne infection causes endocarditis, renal furuncles, and osteomyelitis
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.