A28-year-old woman presents for evaluation of primary infertility. She has had fewer than four periods per year since menarche at age 14, facial hirsutism, acne, and weight gain. On examination, she has a BP 150/100. Her body mass index (BMI) is 40. Acanthosis nigricans is noted along the posterior surface of her neck.
Which of the following laboratory studies is most likely to be abnormal in this patient?
A. TSH
B. prolactin
C. glucose tolerance test
D. growth hormone
E. cosyntropin (Cortrosyn) stimulation test
Correct Answer: C Section: (none)
Explanation: The patient has the typical features of PCOS associated with insulin resistance and the metabolic syndrome. The presence of hyperandrogenism and oligomenorrhea, without other known causes (such as congenital adrenal hyperplasia), makes the diagnosis of PCOS. The hirsutism and acne are the result of the hyperandrogenism associated with PCOS. Thyroid disorders and hyperprolactinemia can contribute to menstrual disturbances but would not be expected to cause the signs of androgen excess or A. nigricans. A cosyntropin stimulation test would be used for the diagnosis of adrenal insufficiency. Growth hormone levels may be elevated in acromegaly or in some pituitary tumors. Women with PCOS have a high risk of glucose intolerance, diabetes, dyslipidemia, and hypertension. Individuals with insulin resistance syndromes typically exhibit hypertriglyceridemia with low HDLlevels. The key to management of PCOS is weight loss. Even modest weight loss (1020 lbs) can result in significant improvement in metabolic and physiologic parameters, such as blood pressure and insulin resistance, and improved fertility.
Question 702:
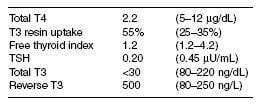
A 60-year-old man with a history of severe chronic obstructive pulmonary disease (COPD), which is steroid dependent, is admitted to the ICU with pulmonary infiltrates and a sepsis syndrome. His hospital course is complicated by acute renal insufficiency and respiratory failure. Therapy includes glucocorticoids and dopamine. He has no history of thyroid disease. Several weeks into his hospital course, the following laboratory studies are performed:
Based on these laboratory studies, which of the following is the most appropriate next step?
A. initiate levothyroxine therapy
B. discontinue glucocorticoid therapy
C. initiate methimazole therapy
D. order MRI of the pituitary
E. supportive treatment only
Correct Answer: E Section: (none)
Explanation:
The patient exhibits the typical features of the nonthyroidal illness syndrome. The total thyroxine level is low, but TBG is also low (based on the elevated T3 resin uptake), so that the free thyroid index is still in the normal range. The low TBG is related to the patient's nutritional deficiency. The low T3 and TSH levels are related to his illness and the use of both glucocorticoids and dopamine, which decrease TSH. The reverse T3 level is high because of the blockade of T4 to T3 conversion caused by the illness. This finding excludes hypopituitarism as an underlying cause. There is no specific therapy for this problem other than treating the underlying illness.
Question 703:
A 19-year-old woman who is 2 months postpartum complains of palpitations, heat intolerance, tremulousness, weight loss, and fatigue. Her thyroid is prominent and firm but nontender. Serum TSH level was undetectable. A nuclear medicine radioactive iodine uptake is performed and shows no uptake of iodine in the neck.
Which of the following is the most appropriate next step?
A. administer radioactive iodine
B. initiate glucocorticoid therapy
C. initiate levothyroxine therapy
D. initiate propranolol therapy
E. initiate methimazole therapy
Correct Answer: D Section: (none)
Explanation:
The patient has the clinical features of hyperthyroidism due to postpartum thyroiditis. This is caused by an autoimmune process with leakage of stored thyroid hormone from the gland. The hyperthyroidism is self-limited and is not associated with new synthesis of thyroid hormone. Therefore, methimazole is not indicated. The thyroid is not painful, as it is in subacute (de Quervain) thyroiditis, so glucocorticoids are not indicated. The radioactive iodine uptake is low, so radioactive iodine treatment is not indicated. Symptom control with propranolol is the only therapy needed during this phase of the illness.
Question 704:
A 54-year-old man presents with a 3-cm right thyroid nodule that was found incidentally by the patient while shaving. He denies any pain or discomfort. He denies any history of thyroid disease, any family history of thyroid disease, and any history of head/neck irradiation. He notes a 10-lb weight loss over the past 6 months. His examination is only remarkable for the firm right thyroid nodule. The remainder of the thyroid is not palpable. There is no adenopathy. Heart rate is 90/minute and regular. The skin is warm and moist, and a fine tremor is present when he holds his hands out. TSH level is <.02 U/mL.
Which of the following is the most appropriate next step?
A. thyroid ultrasound
B. antithyroid peroxidase antibodies
C. thyroid-stimulating immunoglobulins
D. fine needle aspiration of the nodule
E. thyroid nuclear scan
Correct Answer: E Section: (none)
Explanation:
The very low TSH suggests that the patient is hyperthyroid, most likely because of an autonomously functioning thyroid adenoma or hot nodule. In general, these nodules are more than 3 cm in diameter in order to be associated with hyperthyroidism. They are associated with a very low rate of malignancy and do not require fine needle aspiration. The diagnosis would be confirmed by the finding of uptake in the area of the nodule on scan with suppression of uptake in the rest of the thyroid.
Question 705:
A 23-year-old pregnant woman with type 1 diabetes was admitted to the Obstetrics service for DKA. The DKA was appropriately treated and has resolved. You were consulted for medical management of the diabetes, as her sugars have been labile throughout the hospital stay. Your history and review of records reveals that the patient has a long-standing history of noncompliance with diet and medication regimens. She currently uses any insulin she can get and does not eat regular meals. She has fluctuating blood sugars with episodes of hypoglycemia. You counsel the patient extensively, order nutrition and diabetic teaching consults, and discuss keeping home glucose logs. Assuming the patient will follow your advice, which regimen would you recommend to minimize fluctuating glucose readings?
A. NPH insulin twice daily
B. insulin glargine once daily and insulin lispro before meals
C. Humulin 70/30 twice daily
D. NPH twice daily and regular insulin three times daily with meals
E. insulin glargine twice daily
Correct Answer: B Section: (none)
Explanation:
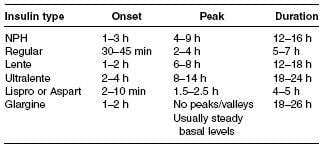
See Table below for onset, peak, and duration of the various types of insulin.
Multiple randomized-controlled trials have shown that tight blood sugar control type I diabetics will reduce the risk of micro-and macrovascular complications, such as retinopathy, neuropathy, and cardiovascular disease. The Diabetes Control and Complications Trial (DCCT) showed that, compared with conventional therapy, intensive therapy significantly reduced the risk of retinopathy progression and clinical neuropathy. Other studies have shown that intensive therapy prevented one cardiovascular event for every 25 patients treated over a 10-year period in a relatively young group of patients. Intensive therapy is not without risk, however. The risk of severe hypoglycemia and subsequent coma or seizure was significantly higher in the intensive therapy group. Control of type I diabetes is dependent on controlling diet with regular low fat meals, keeping blood sugar logs (fasting/ preprandial and postprandial) and adherence to insulin. In type I diabetes, oral hypoglycemics are not useful, as patients have a lack of endogenous insulin production. Most oral hypoglycemic agents work either as insulin sensitizers, secretagogues, or a combination. Type I diabetics need insulin for glycemic control and for prevention of ketoacidosis. Patient acceptance and compliance is critical, for which education is key. Patients must be taught the implications of poor control, and the means to optimize control. Blood sugar testing techniques and nutrition counseling are essential features of success. Regular cardiovascular exercise is also of paramount importance. For patients with poor diet regimens, medication compliance, and blood sugar testing, a longacting agent without peaks and valleys of insulin levels would be an ideal agent for basal insulin. For patients who have no regular mealtimes and history of hypoglycemia, rapidacting insulin is taken at the time of meals is recommended. Patients should also be taught to count carbohydrates and adjust the insulin accordingly (1 g carbohydrate = 1 unit of lispro).
Another option is to use a sliding scale for the lispro based on the premeal sugar levels (using 1 unit for every 3050 mg/dL that the blood sugar is above target). Thus, based on these recommendations, the best option for this patient would be to use insulin glargine as the basal insulin and insulin lispro at the time of meals. However, regular follow-up and compliance with lifestyle measures are key to achieve optimal short-and long-term control and reduction of complications.
Question 706:
A 74-year-old male with a history of hypertension, type II diabetes, myopia, and cataract surgery 2 weeks ago presents with the sudden onset of severe flashes of light and multiple new floaters in his right eye. He denies photophobia, ocular trauma, or diplopia. He also states that he feels as if there is a curtain lowering over his right eye. Your examination and a stat ophthalmology consultation confirm your clinical diagnosis. Of the choices listed below, what would be the most appropriate next step to provide definite treatment for this patient?
A. lens removal and surgical replacement
B. corneal transplant
C. removal of vitreous humor (posterior vitrectomy)
D. intraocular antibiotics
E. stat angiogram and thrombolytics if needed
Correct Answer: C Section: (none)
Explanation:
Retinal detachment is fairly uncommon but should be considered for any patient with visual loss. Risk factors for retinal detachment include advanced age, myopia, cataract surgery, focal retinal atrophy, congenital eye diseases, fibromuscular hyperplasia (FMH) retinal detachment, prematurity, uveitis, diabetic retinopathy, and hereditary vitreoretinopathy. Patients may be asymptomatic but usually present with sudden onset of flashes of light, new floaters, visual field defects, and a sensation of a "curtain" coming down over their visual field. Prompt ophthalmology evaluation, preferably by a retinal specialist, is warranted. Immediate care is paramount as often retinal tears can be managed so as to prevent retinal detachment. Symptomatic retinal tears can be managed with laser or cryo burns to create a chorioretinal scar that prevents fluid access to the subretinal space. This is effective 95% of the time to prevent progression to a retinal detachment. Retinal detachment can be surgically corrected with scleral buckling techniques (90% success rate) or posterior vitrectomy (7590% success rate).
Question 707:
A 74-year-old male with a history of hypertension, type II diabetes, myopia, and cataract surgery 2 weeks ago presents with the sudden onset of severe flashes of light and multiple new floaters in his right eye. He denies photophobia, ocular trauma, or diplopia. He also states that he feels as if there is a curtain lowering over his right eye. What is the most likely cause of his symptoms?
A. central retinal artery occlusion
B. acute lens displacement
C. iritis
D. retinal detachment
E. staphylococcal endophthalmitis
Correct Answer: D Section: (none)
Explanation:
Retinal detachment is fairly uncommon but should be considered for any patient with visual loss. Risk factors for retinal detachment include advanced age, myopia, cataract surgery, focal retinal atrophy, congenital eye diseases, fibromuscular hyperplasia (FMH) retinal detachment, prematurity, uveitis, diabetic retinopathy, and hereditary vitreoretinopathy. Patients may be asymptomatic but usually present with sudden onset of flashes of light, new floaters, visual field defects, and a sensation of a "curtain" coming down over their visual field. Prompt ophthalmology evaluation, preferably by a retinal specialist, is warranted. Immediate care is paramount as often retinal tears can be managed so as to prevent retinal detachment. Symptomatic retinal tears can be managed with laser or cryo burns to create a chorioretinal scar that prevents fluid access to the subretinal space. This is effective 95% of the time to prevent progression to a retinal detachment. Retinal detachment can be surgically corrected with scleral buckling techniques (90% success rate) or posterior vitrectomy (7590% success rate).
Question 708:
A 32-year-old woman complains of episodic confusion in the morning for the past 6 months. During one of these episodes, she was brought to the ER and her serum glucose was found to be 40 mg/dL. She was given intravenous dextrose and her symptoms resolved within 15 minutes. She has gained approximately 25 lbs during the past year. Which of the following would be the most appropriate next step?
A. measure serum insulin and proinsulin 2 hours after a mixed meal
B. MRI of the pancreas
C. measure insulin, C-peptide, and sulfonylurea level on the initial blood sample in ER
D. octreotide scan
E. advise a high protein diet with frequent feedings
Correct Answer: C Section: (none)
Explanation:
The patient appears to have significant hypoglycemia and neuroglycopenia. The differential diagnosis includes medications such as sulfonylureas; alcohol; endocrine deficiency syndromes such as adrenal insufficiency, hypopituitarism, and hypothyroidism; surreptitious insulin administration; and insulinoma. The best way to establish the diagnosis is to measure the levels of each of these levels on the critical sample demonstrating hypoglycemia.
Question 709:
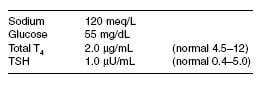
A 40-year-old woman presents with nausea, vomiting, and weakness. She has been amenorrheic since the birth of her last child 1 year ago and has not felt well since that time. On examination, she appears chronically ill, her thyroid is not palpable, and there is no galactorrhea. Laboratory studies on admission include:
The most appropriate next step is to start treatment with which of the following?
A. hydrocortisone
B. fluid restriction
C. desmopressin
D. glucagon
E. fludrocortisone
Correct Answer: A Section: (none)
Explanation:
The patient has Sheehan syndrome, necrosis of the pituitary associated with childbirth. She has panhypopituitarism, but the most urgent hormone to replace is hydrocortisone. Thyroid hormone should not be replaced until after glucocorticoids are administered. The hyponatremia will correct with glucocorticoids and saline. The patient is not deficient in mineralocorticoids, as she does not have primary adrenal insufficiency; therefore, fludrocortisone is not indicated.
Question 710:
A 32-year-old woman presents with complaints of irritability, heat intolerance, hyperdefecation, and frequent palpitations. She has lost 20 lb over the past six months. She has always been in good health and does not take any prescription or OTC medications. She denies any prior history of thyroid disease or exposure to head/neck irradiation, but she states that one of her relatives was diagnosed with a thyroid disorder at roughly the same age. Vital signs are as follows: BP 138/78, HR 112, RR 22, temp. 98.8°F. On examination, her thyroid is diffusely enlarged and smooth. Auscultation of the thyroid reveals a bruit. Her hair is fine in texture, and she has warm velvety skin. She has hyperactive deep tendon reflexes. There is a fine tremor in her outstretched hands.
Which of the following interventions is most appropriate at this time?
A. propylthiouracil
B. thyroidectomy
C. radioactive iodine therapy
D. propranolol
E. potassium iodide
Correct Answer: A Section: (none)
Explanation:
This patient's presentation is consistent with Graves' disease. Infiltrative ophthalmopathy is a common finding in this condition. Approximately 2040% of patients with Graves' disease possess clinically evident eye disease. Complaints include photophobia, diplopia, reduced visual acuity, and easy tearing; and, signs of corneal or conjunctival irritation are oftentimes present. Periorbital edema, chemosis, lid retraction with restricted ocular movement, proptosis, and upward gaze impairment may also be found. Optic nerve compression may also arise, leading to decreased visual acuity, visual field defects, impaired color vision, and papilledema. Macroglossia, hyperkeratosis, cerebellar ataxia, and pericardial effusion are all findings in hypothyroidism. (Ceci Textbook of Medicine, pp. 13961400) Free T3 levels are elevated in all patients with Graves' disease. Most patients also have elevated free T4 levels, but occasionally this level will remain within the normal reference range in a state known as T3 toxicosis. This generally occurs during the initial phases of Graves' disease or at the onset of a relapse. TSH levels are suppressed by the elevated thyroid hormone levels.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.