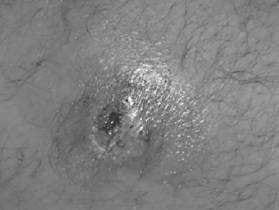
A23-year-old presents with the history of a suspected spider bite to the left groin. On questioning, no one saw a spider. The patient has been healthy except occasional boils under his arms and in the groin. The patient is afebrile. No family members are sick.
Appropriate treatment would include which of the following?
A. Benadryl and topical steroids
B. surgical debridement
C. incision and drainage
D. treatment with TMP-SMZ
E. observation and instructions to the patient to pop any pustules to help it drain
Correct Answer: D Section: (none)
Explanation:
Above shows a pustule or furuncle with a necrotic center. With the patient having a history of boils under his arms and groin, a S. aureus infection should be suspected. Communityacquired methicillin-resistant S. aureus (MRSA) infection has been described to present as an appearance similar to a spider bite. Brown recluse spider bites have necrotic centers, but do not usually form pustules. TMP-SMZ is the best oral agent available for MRSA. Benadryl and topical steroids would not be indicated. Surgical debridement is not indicated. If there is a large pustule, incision and drainage of the wound may be useful. Alternatively, a needle aspirant of drainage could be sent for culture. Patients should be instructed not to press on these lesions to express puss. This causes bacterimia and can later lead to serious systemic infections due to S. aureus. If a patient with S. aureus infection becomes febrile, he should be admitted to the hospital for systemic antibiotics. Blood cultures should be taken. S. aureus easily forms abscesses in the skin and in other tissues. Blood-borne infection causes endocarditis, renal furuncles, and osteomyelitis.
Question 692:
An 18-year-old female presents for evaluation of facial acne. On examination, she has multiple comedones, papules, and pustules on her forehead, nose, cheeks, and chin. She also has several distinct nodules, each greater than 5 mm in diameter. After 6 months of appropriate treatment, the severity of your patient's acne remains essentially unchanged. You rule out several potential causes for the patient's recalcitrant acne and decide that more aggressive therapy is warranted. As you discuss this option with your patient, which of the following side effects of the proposed treatment necessitates extensive counseling prior to initiation of therapy?
A. pseudotumor cerebri
B. teratogenicity
C. hepatotoxicity
D. nephrotoxicity
E. cardiotoxicity
Correct Answer: B Section: (none)
Explanation:
This patient has nodulocystic acne which is characterized by the presence of multiple comedones, inflammatory papules, pustules, and large nodules. Characteristically, the nodules measure greater than 5 mm in diameter. Initial therapy should include a systemic antibiotic such as tetracycline or erythromycin. Use of local therapy alone may be adequate in individuals with comedonal acne. In cases of acne which feature more of an inflammatory component (with papules and pustules), topical and oral antibiotics are useful. Oral isotretinoin is indicated for severe nodulocystic acne that is unresponsive to other therapies.
Question 693:
An 18-year-old female presents for evaluation of facial acne. On examination, she has multiple comedones, papules, and pustules on her forehead, nose, cheeks, and chin. She also has several distinct nodules, each greater than 5 mm in diameter. Which of the following is most appropriate for initial inclusion in a regimen to treat this patient's acne?
A. erythromycin gel
B. tretinoin 0.025% cream
C. clindamycin lotion
D. oral tetracycline
E. oral isotretinoin
Correct Answer: D Section: (none)
Explanation:
This patient has nodulocystic acne which is characterized by the presence of multiple comedones, inflammatory papules, pustules, and large nodules. Characteristically, the nodules measure greater than 5 mm in diameter. Initial therapy should include a systemic antibiotic such as tetracycline or erythromycin. Use of local therapy alone may be adequate in individuals with comedonal acne. In cases of acne which feature more of an inflammatory component (with papules and pustules), topical and oral antibiotics are useful. Oral isotretinoin is indicated for severe nodulocystic acne that is unresponsive to other therapies.
Question 694:
A 58-year-old male presents to your office for a well-male examination. It has been several years since he last visited a doctor, but he states that he has been in "excellent health." He denies any history of drinking, smoking, or using illegal drugs. He maintains a diet low in sodium and fat. An avid sports enthusiast, he also spends at least 2 hours per day engaged in some type of outdoor physical activity. On physical examination, you discover a translucent waxy papule with raised borders on the posterior aspect of his left shoulder. The treatment modality associated with the lowest recurrence rate is which of these?
A. radiation therapy
B. Mohs micrographic surgery
C. surgical excision
D. electrodesiccation with curettage
E. cryotherapy
Correct Answer: B Section: (none)
Explanation:
Nonmelanoma skin cancer is the most common cancer in the United States. Of this group of cancers, approximately 7080% are basal cell carcinomas (BCC). The majority of the remaining 2030% are squamous cell carcinomas (SCC). Metastasis is less common in BCC than SCC, with an estimated risk for metastasis of less than 0.1%. There is no evidence that total body skin examination reduces morbidity or mortality associated with BCC. The cure rate of BCC ranges anywhere from 80 to 99% depending on the treatment modality employed. Despite adequate treatment, individuals with a prior BCC lesion are at increased risk for development of a subsequent BCC (with a 40% risk of development 35 years after treatment).
The most important risk factor for development of BCC is exposure to UVB (or shortwavelength ultraviolet) radiation. There is some evidence, however, that UVA (or longwavelength ultraviolet) radiation also confers a risk. Sporadic, intense episodes of sun exposure, particularly during childhood, are associated with increased risk of BCC development later in life. Conversely, SCC is apparently associated with cumulative sun exposure, regardless of intensity. Other risk factors implicated in BCC development include arsenic exposure, immunosuppression, exposure to other forms of radiation, and the presence of other skin-affecting conditions such as xeroderma pigmentosum and basal cell nevus syndrome.
Question 695:
A 58-year-old male presents to your office for a well-male examination. It has been several years since he last visited a doctor, but he states that he has been in "excellent health." He denies any history of drinking, smoking, or using illegal drugs. He maintains a diet low in sodium and fat. An avid sports enthusiast, he also spends at least 2 hours per day engaged in some type of outdoor physical activity. On physical examination, you discover a translucent waxy papule with raised borders on the posterior aspect of his left shoulder.
Which of the following is the most important risk factor for development of this skin condition?
A. immunosuppression
B. presence of a chronic inflammatory skin condition
C. chronic arsenic exposure
D. exposure to long-wavelength ultraviolet radiation
E. exposure to short-wavelength ultraviolet radiation
Correct Answer: E Section: (none)
Explanation:
Nonmelanoma skin cancer is the most common cancer in the United States. Of this group of cancers, approximately 7080% are basal cell carcinomas (BCC). The majority of the remaining 2030% are squamous cell carcinomas (SCC). Metastasis is less common in BCC than SCC, with an estimated risk for metastasis of less than 0.1%. There is no evidence that total body skin examination reduces morbidity or mortality associated with BCC. The cure rate of BCC ranges anywhere from 80 to 99% depending on the treatment modality employed. Despite adequate treatment, individuals with a prior BCC lesion are at increased risk for development of a subsequent BCC (with a 40% risk of development 35 years after treatment).
The most important risk factor for development of BCC is exposure to UVB (or shortwavelength ultraviolet) radiation. There is some evidence, however, that UVA (or longwavelength ultraviolet) radiation also confers a risk. Sporadic, intense episodes of sun exposure, particularly during childhood, are associated with increased risk of BCC development later in life. Conversely, SCC is apparently associated with cumulative sun exposure, regardless of intensity. Other risk factors implicated in BCC development include arsenic exposure, immunosuppression, exposure to other forms of radiation, and the presence of other skin-affecting conditions such as xeroderma pigmentosum and basal cell nevus syndrome.
Question 696:
A 58-year-old male presents to your office for a well-male examination. It has been several years since he last visited a doctor, but he states that he has been in "excellent health." He denies any history of drinking, smoking, or using illegal drugs. He maintains a diet low in sodium and fat. An avid sports enthusiast, he also spends at least 2 hours per day engaged in some type of outdoor physical activity. On physical examination, you discover a translucent waxy papule with raised borders on the posterior aspect of his left shoulder.
Which of the following is true of this patient's skin condition?
A. It is the most common malignancy in the United States.
B. Total body skin examination reduces the morbidity and mortality associated with this condition.
C. Metastasis is common.
D. The cure rate is approximately 50%.
E. If appropriately treated, the rate of recurrence (development of a second lesion) is equal to that found in the general population.
Correct Answer: A Section: (none)
Explanation:
Nonmelanoma skin cancer is the most common cancer in the United States. Of this group of cancers, approximately 7080% are basal cell carcinomas (BCC). The majority of the remaining 2030% are squamous cell carcinomas (SCC). Metastasis is less common in BCC than SCC, with an estimated risk for metastasis of less than 0.1%. There is no evidence that total body skin examination reduces morbidity or mortality associated with BCC. The cure rate of BCC ranges anywhere from 80 to 99% depending on the treatment modality employed. Despite adequate treatment, individuals with a prior BCC lesion are at increased risk for development of a subsequent BCC (with a 40% risk of development 35 years after treatment).
The most important risk factor for development of BCC is exposure to UVB (or shortwavelength ultraviolet) radiation. There is some evidence, however, that UVA (or longwavelength ultraviolet) radiation also confers a risk. Sporadic, intense episodes of sun exposure, particularly during childhood, are associated with increased risk of BCC development later in life. Conversely, SCC is apparently associated with cumulative sun exposure, regardless of intensity. Other risk factors implicated in BCC development include arsenic exposure, immunosuppression, exposure to other forms of radiation, and the presence of other skin-affecting conditions such as xeroderma pigmentosum and basal cell nevus syndrome.
Question 697:
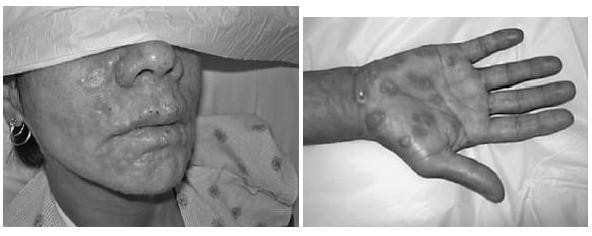
A 34-year-old female sex worker presents with a several week history of fatigue, malaise, fever, and a 10lb weight loss. Over the last 2 weeks, the patient noted a rash on her face, torso, arms, legs, palms, and soles. The patient is HIV negative on a test 2 months ago, has had hepatitis B, gonorrhea, and chlamydia. The patient has an oral temperature of 100.6°F, and generalized lymphadenopathy. The patient does not have any lesions in the mucous membranes.
What is the appropriate treatment?
A. benzathine penicillin 2.4 million units IM weekly for 3 weeks
B. azythromycin 1 g orally
C. aqueous penicillin 4 million units intravenously every 4 hours for 14 days
D. doxycycline 100 mg twice a day for 2 weeks
E. oral corticosteroids over 5 days
Correct Answer: A Section: (none)
Explanation:
The skin lesions as shown in Figures show erythematous maculopapular lesions. There are only a few conditions that cause a rash on the palms and soles. These include syphilis, gonorrhea, and Stevens-Johnson syndrome. Disseminated gonnorhea does not cause lesions on the face. This is not a potential presentation of hepatitis B or chlamydia. Askin biopsy is not indicated. RPR and MHA-TP tests will be positive in syphilis in a high titer. All patients with syphilis need to have HIV testing. The rash of primary HIV infection is a faint erythematous rash on the trunk and is not always present. Early in primary HIV infection, a PCR determination can be negative. In the absence of neurosyphilis, benzthine penicillin 2.4 million units IM weekly for 3 weeks is the treatment of choice for patients with syphilis of unknown duration or greater than a year. While azithromycin 1 g orally will treat gonorrhea and chlamydia, it will not treat syphilis. Aqueous penicillin 4 million units intravenously every 4 hours for 14 days is the treatment of choice for neurosyphilis. An alternate treatment for latent syphilis in patients who are penicillin allergic is doxycycline 100 mg twice daily for 30 days. Oral corticosteroids are not indicated in this case.
Question 698:
A 34-year-old female sex worker presents with a several week history of fatigue, malaise, fever, and a 10lb weight loss. Over the last 2 weeks, the patient noted a rash on her face, torso, arms, legs, palms, and soles. The patient is HIV negative on a test 2 months ago, has had hepatitis B, gonorrhea, and chlamydia. The patient has an oral temperature of 100.6°F, and generalized lymphadenopathy. The patient does not have any lesions in the mucous membranes.
What is the diagnostic test most likely to explain this clinical presentation?
A. a hepatitis B surface antigen test
B. cervical smear for rapid tests for gonorrhea and chlamydiae
C. a skin biopsy
D. a rapid plasma reagin (RPR) and microhemagglutination assay for Treponema pallidum (MHA-TP) test
E. an HIV viral load by polymerase chain reaction (PCR)
Correct Answer: D Section: (none)
Explanation:
The skin lesions as shown in Figures show erythematous maculopapular lesions. There are only a few conditions that cause a rash on the palms and soles. These include syphilis, gonorrhea, and Stevens-Johnson syndrome. Disseminated gonnorhea does not cause lesions on the face. This is not a potential presentation of hepatitis B or chlamydia. Askin biopsy is not indicated. RPR and MHA-TP tests will be positive in syphilis in a high titer. All patients with syphilis need to have HIV testing. The rash of primary HIV infection is a faint erythematous rash on the trunk and is not always present. Early in primary HIV infection, a PCR determination can be negative. In the absence of neurosyphilis, benzthine penicillin 2.4 million units IM weekly for 3 weeks is the treatment of choice for patients with syphilis of unknown duration or greater than a year. While azithromycin 1 g orally will treat gonorrhea and chlamydia, it will not treat syphilis. Aqueous penicillin 4 million units intravenously every 4 hours for 14 days is the treatment of choice for neurosyphilis. An alternate treatment for latent syphilis in patients who are penicillin allergic is doxycycline 100 mg twice daily for 30 days. Oral corticosteroids are not indicated in this case.
Question 699:
A28-year-old woman presents for evaluation of primary infertility. She has had fewer than four periods per year since menarche at age 14, facial hirsutism, acne, and weight gain. On examination, she has a BP 150/100. Her body mass index (BMI) is 40. Acanthosis nigricans is noted along the posterior surface of her neck. How would you counsel this patient?
A. The primary treatment for this problem is with medications.
B. Weight loss is key to her management.
C. Her hypertension would be best treated with a thiazide diuretic.
D. Regardless of her lipid panel result, she should be on a statin.
E. Her infertility is due to lack of estrogen production.
Correct Answer: B Section: (none)
Explanation: The patient has the typical features of PCOS associated with insulin resistance and the metabolic syndrome. The presence of hyperandrogenism and oligomenorrhea, without other known causes (such as congenital adrenal hyperplasia), makes the diagnosis of PCOS. The hirsutism and acne are the result of the hyperandrogenism associated with PCOS. Thyroid disorders and hyperprolactinemia can contribute to menstrual disturbances but would not be expected to cause the signs of androgen excess or A. nigricans. A cosyntropin stimulation test would be used for the diagnosis of adrenal insufficiency. Growth hormone levels may be elevated in acromegaly or in some pituitary tumors. Women with PCOS have a high risk of glucose intolerance, diabetes, dyslipidemia, and hypertension. Individuals with insulin resistance syndromes typically exhibit hypertriglyceridemia with low HDLlevels. The key to management of PCOS is weight loss. Even modest weight loss (1020 lbs) can result in significant improvement in metabolic and physiologic parameters, such as blood pressure and insulin resistance, and improved fertility
Question 700:
A28-year-old woman presents for evaluation of primary infertility. She has had fewer than four periods per year since menarche at age 14, facial hirsutism, acne, and weight gain. On examination, she has a BP 150/100. Her body mass index (BMI) is 40. Acanthosis nigricans is noted along the posterior surface of her neck. Which of the following would be her most likely fasting lipid profile?
A. high TGs, high HDL
B. low TGs, low HDL
C. high TGs, low HDL
D. high LDL cholesterol
E. normal lipid profile
Correct Answer: C Section: (none)
Explanation:
The patient has the typical features of PCOS associated with insulin resistance and the metabolic syndrome. The presence of hyperandrogenism and oligomenorrhea, without other known causes (such as congenital adrenal hyperplasia), makes the diagnosis of PCOS. The hirsutism and acne are the result of the hyperandrogenism associated with PCOS. Thyroid disorders and hyperprolactinemia can contribute to menstrual disturbances but would not be expected to cause the signs of androgen excess or A. nigricans. A cosyntropin stimulation test would be used for the diagnosis of adrenal insufficiency. Growth hormone levels may be elevated in acromegaly or in some pituitary tumors. Women with PCOS have a high risk of glucose intolerance, diabetes, dyslipidemia, and hypertension. Individuals with insulin resistance syndromes typically exhibit hypertriglyceridemia with low HDLlevels. The key to management of PCOS is weight loss. Even modest weight loss (1020 lbs) can result in significant improvement in metabolic and physiologic parameters, such as blood pressure and insulin resistance, and improved fertility
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.