A 32-year-old woman presents with complaints of irritability, heat intolerance, hyperdefecation, and frequent palpitations. She has lost 20 lb over the past six months. She has always been in good health and does not take any prescription or OTC medications. She denies any prior history of thyroid disease or exposure to head/neck irradiation, but she states that one of her relatives was diagnosed with a thyroid disorder at roughly the same age. Vital signs are as follows: BP 138/78, HR 112, RR 22, temp. 98.8°F. On examination, her thyroid is diffusely enlarged and smooth. Auscultation of the thyroid reveals a bruit. Her hair is fine in texture, and she has warm velvety skin. She has hyperactive deep tendon reflexes. There is a fine tremor in her outstretched hands.
Which of the following sets of laboratory results would be consistent with this patient's presentation?
TSH free T3 free T4
A. low lowhigh
B. low normal normal
C. low high high
D. highlow low
E. high high high
Correct Answer: C Section: (none)
Explanation:
This patient's presentation is consistent with Graves' disease. Infiltrative ophthalmopathy is a common finding in this condition. Approximately 2040% of patients with Graves' disease possess clinically evident eye disease. Complaints include photophobia, diplopia, reduced visual acuity, and easy tearing; and, signs of corneal or conjunctival irritation are oftentimes present. Periorbital edema, chemosis, lid retraction with restricted ocular movement, proptosis, and upward gaze impairment may also be found. Optic nerve compression may also arise, leading to decreased visual acuity, visual field defects, impaired color vision, and papilledema. Macroglossia, hyperkeratosis, cerebellar ataxia, and pericardial effusion are all findings in hypothyroidism. (Ceci Textbook of Medicine, pp. 13961400) Free T3 levels are elevated in all patients with Graves' disease. Most patients also have elevated free T4 levels, but occasionally this level will remain within the normal reference range in a state known as T3 toxicosis. This generally occurs during the initial phases of Graves' disease or at the onset of a relapse. TSH levels are suppressed by the elevated thyroid hormone levels.
Question 712:
A 32-year-old woman presents with complaints of irritability, heat intolerance, hyperdefecation, and frequent palpitations. She has lost 20 lb over the past six months. She has always been in good health and does not take any prescription or OTC medications. She denies any prior history of thyroid disease or exposure to head/neck irradiation, but she states that one of her relatives was diagnosed with a thyroid disorder at roughly the same age. Vital signs are as follows: BP 138/78, HR 112, RR 22, temp. 98.8°F. On examination, her thyroid is diffusely enlarged and smooth. Auscultation of the thyroid reveals a bruit. Her hair is fine in texture, and she has warm velvety skin. She has hyperactive deep tendon reflexes. There is a fine tremor in her outstretched hands. Which of the following is a common finding in this condition?
A. macroglossia
B. hyperkeratosis
C. infiltrative ophthalmopathy
D. cerebellar ataxia
E. pericardial effusion
Correct Answer: C Section: (none)
Explanation:
This patient's presentation is consistent with Graves' disease. Infiltrative ophthalmopathy is a common finding in this condition. Approximately 2040% of patients with Graves' disease possess clinically evident eye disease. Complaints include photophobia, diplopia, reduced visual acuity, and easy tearing; and, signs of corneal or conjunctival irritation are oftentimes present. Periorbital edema, chemosis, lid retraction with restricted ocular movement, proptosis, and upward gaze impairment may also be found. Optic nerve compression may also arise, leading to decreased visual acuity, visual field defects, impaired color vision, and papilledema. Macroglossia, hyperkeratosis, cerebellar ataxia, and pericardial effusion are all findings in hypothyroidism. (Ceci Textbook of Medicine, pp. 13961400) Free T3 levels are elevated in all patients with Graves' disease. Most patients also have elevated free T4 levels, but occasionally this level will remain within the normal reference range in a state known as T3 toxicosis. This generally occurs during the initial phases of Graves' disease or at the onset of a relapse. TSH levels are suppressed by the elevated thyroid hormone levels.
Question 713:
A34-year-old woman was found to have a 2-cm right thyroid nodule at the time of a well woman examination. The remainder of the thyroid was palpably normal and there were no lymph nodes palpable. There was no history of thyroid disease or radiation therapy to her head or neck. She was clinically euthyroid. Thyroid-stimulating hormone (TSH) was normal. Which of the following tests would be the most useful in establishing a specific diagnosis?
A. ultrasound of the thyroid
B. nuclear scan of the thyroid
C. thyroid antibody studies
D. fine needle aspiration of the nodule
E. CT of the neck
Correct Answer: D Section: (none)
Explanation:
In evaluating a sporadic thyroid nodule in a patient who is euthyroid, it is critical to determine whether the nodule is malignant or benign. The most diagnostic test is the fine needle aspiration. Ultrasound will only distinguish between cystic and solid structures, and most nodules have some solid component. The nuclear scan will demonstrate a photopenic area in over 85% of patients. Neither these tests nor CT scan will reliably separate benign from malignant nodules. Thyroid antibody studies do not play a role in the evaluation of a thyroid nodule in a euthyroid patient. They are sometimes used in the evaluation of thyroiditis.
Question 714:
Vitamin D supplementation can be helpful in treating which disease?
A. hyperparathyroidism
B. hypoparathyroidism
C. alcoholic neuritis
D. pernicious anemia
E. scurvy
Correct Answer: B Section: (none)
Explanation:
Vitamin D is actually a hormone that, along with parathyroid hormone and calcitonin, regulates plasma calcium concentration. One action of vitamin D is to increase plasma Ca2+, which can be reduced in hypoparathyroidism. Scurvy is associated with vitamin C deficiency. Alcoholic neuritis is associated with thiamine deficiency.
Question 715:
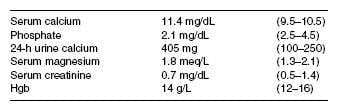
A 58-year-old woman is concerned about her risk for osteoporosis and is seen by her general internist. Her mother was diagnosed with osteoporosis and had a hip fracture at age 84. She has no personal or family history of kidney stones or ulcer disease, and she has never had a fracture. She had a hysterectomy at age 48 and took estradiol for 2 years, but discontinued because of a fear of adverse effects. She does not have any vasomotor symptoms. She takes 1500 mg of calcium carbonate and 400 IU vitamin D daily. She is not on any other medications. On examination, she appears well developed and there is no evidence of kyphosis. ABMD test is performed that demonstrates a T score in the spine of 3.5 and in the hip of 2.8. CXR and mammogram are normal. Further evaluation demonstrates the following: Which of the following is the most likely diagnosis?
A. milk-alkali syndrome
B. primary hyperparathyroidism
C. sarcoidosis
D. secondary hyperparathyroidism
E. osteomalacia
Correct Answer: B Section: (none)
Explanation:
Primary hyperparathyroidism is common in postmenopausal women and more than 80% present without any symptoms. The most common findings are bone loss, usually in association with estrogen deficiency. The elevated calcium, decreased phosphate, and increased urinary calcium are typical of this disorder. Milk-alkali syndrome is primarily historical disease occurring in patients receiving large quantities of calcium and alkali, and presenting with renal insufficiency, elevated phosphate, and alkalosis. Her normal renal function and relatively low dose of calcium exclude this entity. Familial hypocalciuric hypercalcemia is autosomal dominant and is diagnosed by a low urinary calcium clearance. The lack of renal insufficiency excludes secondary hyperparathyroidism. The normal CXR and Hgb make sarcoidosis and multiple myeloma unlikely. Postmenopausal osteoporosis and osteomalacia are excluded by the elevated calcium level.
Question 716:
A 64 year old woman presents with bilateral symmetric arthralgias and morning stiffness for several years. She says that she has been worked up for RA in the past. On review of her records as well as the examination you note subcutaneous nodules, positive rheumatoid factor, and radiographs of the hands that revealed joint erosions. Which of her findings has the highest positive likelihood ratio (LR) for the diagnosis of RA?
A. morning stiffness
B. rheumatoid nodules on examination
C. symmetric arthralgias
D. joint erosions of the hand on xray
E. positive rheumatoid factor.
Correct Answer: D Section: (none)
Explanation:
RA is primarily a clinical diagnosis. The history and physical examination are crucial to confirming the diagnosis and ruling out differential diagnosis. No one laboratory analysis can make the diagnosis, however using laboratory analysis in conjunction with a detailed history and examination can help to confirm the clinical suspicion. Some findings that may suggest RA include: morning stiffness (LR 1.9), symmetric arthralgias (LR 1.2), rheumatoid nodules (LR 3.0), positive serum rheumatoid factor (LR 8.4), and radiographic changes of hands/wrists that demonstrate erosions or hypodensity adjacent to the joints (LR 11). Rheumatoid factor is present in about 70% of patients with the diagnosis at some point in the course, however in less than 30% of patients with early RA. ANAmay be positive in 2040% of RA patients but may also be positive in many other disease states. Anti-CCP antibodies have been reported to have a sensitivity of 4070% and specificity of 95%. The presence of both RF and anti-CCP is very highly specific for the diagnosis of RA
Question 717:
A 42 year old male admitted for pulmonary embolus was placed on heparin, dosed by a weight based protocol. However, later in the day, you receive a call from the floor nurse stating that the patient had spontaneous epistaxis and a very high aPTT. Use of which of the following would be best at this time?
A. cimetidine
B. heparinase
C. clofibrate
D. protamine sulfate
E. vitamin K
Correct Answer: D Section: (none)
Explanation:
Protamine sulfate is a strongly basic molecule that is thought to inhibit acidic heparin electrostatically. It may not, however, affect heparin-induced platelet aggregation. Cimetidine is an H2-antagonist that increases the anticoagulant response by an as yet unknown mechanism. Clofibrate is an agent used to reduce plasma lipid levels. Vitamin K is used to reverse the effect of warfarin. Heparinase is not used clinically.
Question 718:
A62-year-old female with a history of a recent pulmonary embolus presents to your office for follow-up on anticoagulation treatment. She takes warfarin on a daily basis. She reports that for the last week she has noticed mild rectal bleeding and multiple bruises over the extremities with minimal trauma. She is comfortable appearing with normal vital signs and is not orthostatic. You ordered a stat CBC and PT/INR which revealed a mildly decreased Hgb at 11 g/dL and an elevated INR of 7. Which of the following would be the most appropriate intervention?
A. subcutaneous injections of heparin
B. oral allopurinol
C. intravenous protamine sulfate
D. oral vitamin E
E. oral vitamin K
Correct Answer: E Section: (none)
Explanation:
Warfarin acts as a vitamin K antagonist by blocking the regeneration of the reduced form of the vitamin. The result is a decrease in clotting factors II, VII, IX, and X leading to an increase in bleeding time. Warfarin toxicity can be alleviated by increasing the availability of vitamin K.
Question 719:
A 23-year-old woman presents to your acute care clinic with a complaint of fever, sore throat, and malaise
of sudden onset. Her prior medical history is significant for schizophrenia. Her vitals signs are:
BP 116/80, HR 112, RR 26, Temp 100.6 degrees Fahrenheit. On physical examination, her oral cavity
features painful aphthous ulcers as well as swollen gums. Initial laboratory testing includes a CBC which
returns with the following results:
· Leukocyte count 800/mm3
· Hgb 12.1 g/dL
· HCT 37.0%
· Platelet count 212 × 109/L
· Differential:
· Neutrophils, segmented 52%
· Neutrophils, bands 3%
· Lymphocytes 35%
· Monocytes 7%
· Eosinophils 3%
· Basophils 0%
Which of the following best describes the expected course of the patient's condition?
A. The condition is usually self-limiting and requires no intervention.
B. Use of G-CSF has been shown to speed recovery.
C. Dose reduction of the offending agent often leads to resolution of symptoms.
D. If discovered earlier, discontinuation of the offending agent would have prevented progression of the condition to its current severity.
E. Tardive dyskinesia usually develops as a late finding.
Correct Answer: B Section: (none)
Explanation:
This patient's presentation is consistent with agranulocytosis, which is defined by an absolute neutrophil count (ANC) of fewer than 500/mm3. ANC is defined as the percentage of the WBC count that is accounted for by segmented neutrophils and bands. In the case of this patient, the ANC is 55% of the WBC count or 440/mm3. Individuals with agranulocytosis commonly experience a sudden onset of malaise, fever, chills, and pharyngitis. They may also develop painful aphthous ulcers affecting the oropharyngeal mucosa. Suppression of the bone marrow, including agranulocytosis, is associated with the use of clozapine. The incidence approaches 1% within several months of treatment, independent of dose. Patients on clozapine should be monitored closely with weekly measurement of the CBC. Mild leukocytosis and other blood dyscrasias occur much less frequently with other antipsychotic drugs.Usually, there is a prodrome of several weeks duration in which the WBC count gradually declines. Decreasing the dose or discontinuing the offending agent does not always prevent progression to full blown agranulocytosis. Patients with druginduced neutropenia recover more quickly with the assistance of granulocyte colonystimulating factor (G-CSF). Additionally, individuals suffering from agranulocytosis frequently develop infections which require the use of antibiotic therapy. In these cases, further supportive and symptomatic care may be necessary depending on the severity of infection. Delaying or withholding intervention is inappropriate. Tardive dyskinesia is an adverse effect related to use of antipsychotic medications; it is not inherently related to agranulocytosis.
Question 720:
A 23-year-old woman presents to your acute care clinic with a complaint of fever, sore throat, and malaise
of sudden onset. Her prior medical history is significant for schizophrenia. Her vitals signs are:
BP 116/80, HR 112, RR 26, Temp 100.6 degrees Fahrenheit. On physical examination, her oral cavity
features painful aphthous ulcers as well as swollen gums. Initial laboratory testing includes a CBC which
returns with the following results:
· Leukocyte count 800/mm3
· Hgb 12.1 g/dL
· HCT 37.0%
· Platelet count 212 × 109/L
· Differential:
· Neutrophils, segmented 52%
· Neutrophils, bands 3%
· Lymphocytes 35%
· Monocytes 7%
· Eosinophils 3%
· Basophils 0%
Use of which of the following must be considered when formulating a differential diagnosis to explain this patient's symptoms?
A. haloperidol
B. chlorpromazine
C. risperidone
D. thioridazine
E. clozapine
Correct Answer: E Section: (none)
Explanation:
This patient's presentation is consistent with agranulocytosis, which is defined by an absolute neutrophil count (ANC) of fewer than 500/mm3. ANC is defined as the percentage of the WBC count that is accounted for by segmented neutrophils and bands. In the case of this patient, the ANC is 55% of the WBC count or 440/mm3. Individuals with agranulocytosis commonly experience a sudden onset of malaise, fever, chills, and pharyngitis. They may also develop painful aphthous ulcers affecting the oropharyngeal mucosa. Suppression of the bone marrow, including agranulocytosis, is associated with the use of clozapine. The incidence approaches 1% within several months of treatment, independent of dose. Patients on clozapine should be monitored closely with weekly measurement of the CBC. Mild leukocytosis and other blood dyscrasias occur much less frequently with other antipsychotic drugs.Usually, there is a prodrome of several weeks duration in which the WBC count gradually declines. Decreasing the dose or discontinuing the offending agent does not always prevent progression to full blown agranulocytosis. Patients with druginduced neutropenia recover more quickly with the assistance of granulocyte colonystimulating factor (G-CSF). Additionally, individuals suffering from agranulocytosis frequently develop infections which require the use of antibiotic therapy. In these cases, further supportive and symptomatic care may be necessary depending on the severity of infection. Delaying or withholding intervention is inappropriate. Tardive dyskinesia is an adverse effect related to use of antipsychotic medications; it is not inherently related to agranulocytosis.
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.